




Hello everyone.
Greetings from Montecito.
MD and I got back a couple of days ago from the San Diego LowcarbUSA meeting. We had to drive through Hilary the entire way back. It was incredibly frustrating because people who live in Southern California drive through the rain the same way people in Arkansas drive when it snows. Normally here people drive fast zigging in and out of traffic constantly. During the drive from San Diego, all we encountered were people driving at about 45-50 mph with their frigging emergency flashers on. Had this been in a major Texas or Arkansas rain—the kind that blows sideways with a torrential downpour the wipers can’t keep up with even on full speed—then I might understand it. But this was just rain. And not even that hard. And almost no wind.
As you might imagine, it took us forever.
Met a bunch of Arrow readers at the conference and caught up with a lot of old friends. For me that’s the best part of these conferences.
Here I am with Jay Wortman (L), who gave a great talk, and Rod Taylor who runs Lowcarbdownunder in Australia. Thanks to Rod, both MD and I are going to speak at Lowcarbdownunder in October. He had to endure the harrowing ride with me at the wheel between San Diego and LAX, where we dropped him off to catch his flight home.

And here is a photo of me and MD along with Siobhan Huggins on the left, who works with Dave Feldman, Rod Taylor and Belinda Lennertz. Belinda is a pediatric endocrinologist who works with David Ludwig at Harvard. I’ve read all her papers, but had never met her till this conference.

Finally, here is yours truly pontificating from the stage.
I got to see a lot of the talks, but not all. I was going to give roughly the same talk I gave in Boca Raton in January, but at the last minute I decided to change it up a bit. Which ended up changing it a lot and put me under the gun to get the slides all made.
After coming up for air, I now have to start working on the slides for the two talks I’m going to give in Australia in October. And I don’t want to be working on them right up to the last minute as I was here.
It’s stressful to work on them right up till the last, but I think the presentations are much better that way. I had a terrible experience years ago that scarred me for making slides way in advance.
I used to speak at a nutritional conference in Boulder in August every year. Robert Crayhon (RIP) put these together and did a bang-up job of it. I spoke at every one. Robert was always on me (and the other speakers) to get their slides in earlier. Everyone ignored him. Finally, he got pissed and emailed all the scheduled speakers in May or June telling us all we had to get our slides in by July 10 (which I think was a month before the conference that year). He said anyone who didn’t have their slides in his hands by July 10 would be struck from the schedule.
I didn’t want to risk it, so I buried myself in my slides a few days before I had to get them in the overnight to get there by July 10. (This was before the days you could just send a Dropbox link.) Once I got into the Powerpoint program, which I had to relearn every time I used it, I discovered I could animate my slides. It was a new toy, so I went over the top with it.
I got my slides off on time and told MD I was actually glad. That now I didn’t have to stress right up to the time of the meeting as usual. When I showed up for the meeting, I went to the little green room to run through my slides before I went on stage.
When I started flipping through the deck, I realized I didn’t remember all the animations. I went into a blind panic, trying to race through them and figure out when all these arrows and objects were going to come flying in on the slides. My time ran out and I had to go on.
It was horrible. I would talk about whatever slide was on the screen, then move on to the next. But instead of the next slide some arrow came flipping in that expanded on the slide I thought I had just finished explaining. I’m not sure what the audience thought, or if they even realized anything was amiss, but I was a basket case before it was over.
Since then, I have always put off my slide making as long as possible, so it will be fresh in my mind when I make the presentation. [The bride suggested that maybe I make them in advance and then go over them repeatedly in the interval between, but that seems too easy.]
If you would like to attend next year’s LowCarbUSA conference in San Diego, the organizer said we could give our friends a discount code that reduces the price by 40 percent. But only until this coming Monday night, Aug 28. The discount code is ReturningSD. Click here if you’re interested. I would love to meet you. I have no idea what I’m going to talk about, but I’ll figure out something interesting by then.
August 24, 79 AD
1944 years ago today Vesuvius blew. The many, many kilotons of ash and mud rained down killing thousands of people and covering the towns of Pompeii and Herculaneum. I’ve spent a lot of time at both places, Pompeii more than Herculaneum. And I’ve climbed Mount Vesuvius and peered into the crater. If you ever go to that part of Italy, both cities are must-see sights. Peering into Vesuvius not so much. It’s a long run for a short slide.
Here is a video I watch at least once a year. It starts on the morning of August 24, 79 AD before the eruption and runs a timeline thereafter. You can see just what the poor people who lived there had to contend with on a day that started off normal.
If you would like to read an historically accurate (as far as a novel can be historically accurate) account of the eruption, give Robert Harris's Pompeii a go. He meticulously researches all his novels, so I'm sure the timeline--if nothing else--is on the money. Terrifically entertaining and horrific at the same time. You won't be disappointed.
If you ever go to that part of Italy, make sure to see both Pompeii and Herculaneum. If you’ve just got time for one, see Herculaneum. Pompeii is always clotted with tourists. We’ve been there five or six times at various times of the year, and it’s always packed. Herculaneum not so much. I spent an afternoon there with my sister while MD was in rehearsal for one of her tour concerts. There were maybe ten other people there—in the whole place—at most. Herculaneum is considerably smaller than Pompeii, but it has all the same kinds of stuff to see. Whereas Pompeii has dozens, if not hundreds, of what would be considered fast food restaurants, tabernae, Herculaneum might have ten. But if you’ve seen one, you’ve seen them all. They all look exactly the same. If you hate crowds, avoid Pompeii in favor of Herculaneum. [The bride says brave the crowds and see Pompeii; it’s amazing and worth it!]
I’m sure however bad your day was today, it can’t compare to this.
Everything You Believe Is Wrong
Matt Briggs published a book a few years ago with the above title. Now he is putting it online chapter by chapter on his Substack. If you are interested, you can discover all the fallacies used to manipulate you by politicians, the media, Big Tech, Big Pharma, and anyone else in whose interest it is to fool you.
He starts out with pretty simple fallacies we’ve all encountered. These are so common that most of us, me included, would probably not even think of them as fallacies.
One in particular caught my eye. He writes about what he calls “The Non-Fallacy Fallacy” may also be called the “Stubbornness Fallacy” or the “I Can’t Hear You Fallacy.” I can pull another fallacy out of it. One of my own invention.
It happens when you make a decent point or offer a valid argument and your opponent only pretends to have listened or read it. He acts as if he’s discovered an obvious flaw, a mistake not worth his effort to refute. Your argument is brushed away and your opponent moves on.
Bullies like this one. You hear this in interviews with politicians and famous personages. The newsman has just asked a coherent question (it does happen) which if answered truthfully will damn the politician. So the politician sidesteps it. This is so routine I’m embarrassed to even include it because everybody can see through this ploy. The only reason I mention it is exasperation. Why do the newsmen never follow up until they get an answer to their question? Lawyers always do. “Yes or no, Senator…Yes or no, Senator…” Exhaustion and the easy acceptance of lies by our elites is the only explanation I can think of. The British, God bless them, are particularly adept at this fallacy.
Toward the end, Briggs talks about how lawyers bore in on witnesses with the “Yes or no” demands. Which always pisses me off when I see it used. I don’t care who uses it, or whom it is being used upon. I hate it.
Let’s say you were being attacked by an assailant with a chainsaw. You were trying to defend yourself and, in doing so, you threw a rock at him, hit him in the head, and killed him. At some future date, you are being questioned by a lawyer, and you get hit with the “all I want is a yes or no, did you ever kill a man?” When you try to answer that it was in self defense, you get cut off with, “I just want a yes or no; did you ever kill a man?”
Granted, it’s fun to see this used on someone you hate in, say, a congressional hearing. Where you hear it a lot. But ultimately it will be used on someone you like, and you’ll see how unfair it is. I would call this one the Yes or No fallacy.
Other than just that one tiny segment that got me agitated, I think this whole series is great. I bought his book way back when, so I’ve already read all these, but seeing a few of them presented each day will be a nice review.
GLP-1 Agonists Cause Issues For Many People
A reader sent me the video below. I have no idea who this woman is. I’ve never seen one of her videos before, but a whole lot of other people obviously have as she has over two million subscribers to her YouTube channel.
I would encourage you to watch the video if you are considering giving Wegovy, Ozempic, or Mounjaro a try.
What is even more disturbing than the video is the long list of comments—over 6,500—from people, most of whom have had similar or worse outcomes.
In reading through the comments, I came upon one that said Jamie French had had problems as well. I didn’t have a clue who Jamie French was, so I looked her up. She’s another YouTube celeb with almost 750,000 subscribers. She, too, has had major problems with Ozempic.
When I pulled her YouTube up to watch, I noticed a slew of others along the right side of people who were telling their horror stories about these drugs. The YouTube above also has over 6,000 comments from people, again most of whom have had issues with these drugs.
It’s not just these YouTubers who have been affected. Suicidal ideation is known to the companies that make these drugs, but I suspect vastly underreported.
Of more than 1200 reports of adverse reactions with semaglutide, 60 cases of suicidal ideation and seven suicide attempts have been reported since 2018, according to the US Food and Drug Administration's (FDA's) Adverse Event Reporting System (FAERS) public database. For liraglutide, there were 71 cases of suicidal ideation, 28 suicide attempts, and 25 completed suicides out of more than 35,000 reports of adverse reactions. [Links in original.]
As I’ve written over and over in these pages, I am NOT an early adopter when it comes to new drugs. Especially not now when the FDA has become so lax, as I wrote about last week.
I wouldn’t take one of these drugs on a dare. My bet is that the lawsuits will fly before too long. If not, I will be truly surprised.
The situation is troubling, to say the least.
Here is something else I find troubling.
What’s the Truth About the War In Ukraine?
I try to stay away from subjects like this because they are so polarizing. Folks seem to never think critically about these things, but instead simply line up on the side of their political tribe.
I’ve read countless articles on this war from all different perspectives. Everyone seems to have an agenda, so it’s difficult to get answers that can be believed. But I learned something a couple of days ago that has got me really wondering. More about which later.
Tucker Carlson posted a long interview yesterday with Col. Doug McGregor, whom he’s had on his show numerous times back when he had a show. This interview was done on Twitter, so I can’t embed it. I encourage you to watch it, however, just to get a view you’ve probably not gotten before.

Click here to watch on Twitter. Or click on the image above.
Most of the people who are all in on the Ukraine war are the same people who were for mandates, masking, giving kids untested vaccines, lockdowns, etc. They were wrong about all these things, so odds are they are wrong about the war in Ukraine.
But I’ve harbored a hope that the Ukrainians could somehow pull off a win. As I’ve written before, my long-time CPA, who is a very good friend as well, did the forensic accounting work for a company that has been the only company to both successfully sue Vladimir Putin and also actually collect from him. I’ve heard the horror stories from my CPA who went to Russia a number of times during this whole fiasco.
The man who owned the company wrote a book about his experience. It delves into all the routine corruption that is rife in Russia. If you would like to know how Russia operates, I would highly recommend his book. I don’t think Putin is any worse really than anyone else there; he just happened to be in charge when the events in this book took place.
There are reasons to fear Ukraine is even more corrupt than Russia. And I’ve read all kinds of stories about how Zelensky has been moving tons of money—money provided by the US—out of Ukraine and into expensive properties in other parts of the world. Whether they’re true or not, who can say?
In the Tucker interview, Col McGregor says the US would come out badly in a war against Russia. In fact, he thinks we might lose. I think that is insane. I don’t know squat about our military, and I know even less about Russia’s. But I do know that Russia’s economy, as measured by GDP, os a little over $2T per year. The most recent defense budget for the US was $834B, which is a little less than half of Russia’s total GDP. Russia’s GDP is less than Italy’s. I just don’t see the major threat that McGregor sees based on monetary factors alone.
Just to confirm how crappy their graft-laden country is, their moon landing craft blew up. Or, as they reported, it ceased to exist. Who knows if the huge arsenal of nukes they allegedly have would even work?
As I say, aside from all the reading I’ve done on this subject, I don’t feel like I’ve got any kind of real sense as to what’s going on. But I did get some interesting info a few days ago. And I have no idea what it means. Maybe someone reading this can enlighten me.
And now Yevengy Prigozhin, the head of the Wagner group (Russian mercenaries), is dead from a plane crash that obviously wasn’t an accident. You can see it here. This plane pirouetted down. This isn’t how a plane that is in trouble falls. He was killed. But by whom?
https://twitter.com/jacksonhinklle/status/1694397300695556250
Either there was a bomb in the plane, or it was shot down. So Russian. So Putin.
Our middle son just returned from a two week golf trip to Ireland. He went with a fraternity brother from college to celebrate their 50th birthdays. Soon after they got there, they came upon a bunch of young Ukrainian men in a pub. They tried to strike up a conversation with them about what was going on in Ukraine, but the Ukrainians became uncomfortable and said they were going outside to smoke.
When they left, the bartender told our son and his friend that young Ukrainian men had fled from Ukraine and were hiding out all over Ireland and other western European countries. He told them that the Ukrainians were getting their room and board paid for, along with about a $600 per month stipend. Our son asked who was paying for it. The bartender said the EU.
In each place our son and friend stopped in Ireland, the hotels were filled with able-bodied young Ukrainian men on the lam. Which I can understand. Who wants to be cannon fodder? Especially if things are going as McGregor says they are. But why on earth would the EU be paying for them to hide out.
This is the first I’ve heard of this. Our kid witnessed it all over Ireland. He had trouble finding rooms and getting room upgrades on the ones he had because all the hotel rooms were filled with young Ukrainians
Does anyone know anything about this? If so, I’m all ears.
As always, it would really be nice if we had a media we could count on to dig in and investigate these issues instead of just flaking for various politicians.
The Very Model of A Modern Medical Practitioner
Okay, I want to do something a little different here. I’m putting up a video of a very smart doc from Yale giving a lecture on how to treat obesity. She and I have totally different approaches to treating overweight patients. I’m sure her methods work, at least in the short term. But I’m not sure they are optimal for overweight people in the long run, simply because they’ve never been tested for very long.
Her premise, and it is valid, is that obesity is a chronic disease just like type 2 diabetes (T2DM), hypertension, and hyperlipidemia. In her view, if a patient has a chronic disease, it needs to be treated forever. For example, if a patient comes in with hypertension (high blood pressure), then the patient goes out with a prescription for an anti-hypertensive drug and probably a low-salt diet. If blood pressure isn’t down into the normal range by the next visit, she adds another drug. Or changes drugs. Then it’s rinse and repeat until the patient’s blood pressure is under control.
Ditto with T2DM and or elevated cholesterol. Treat with one drug after another until the condition is under control. Once whatever is being treated is under control, she says, you don’t stop treating it. I’ve said the same thing. If you treat a patient with high blood pressure with a drug, and the BP comes down, you don’t stop treatment. If you did and BP went back up, you wouldn’t be surprised.
She makes the point in her talk, which is apparently to medical students, that obesity is a chronic disease just like the others mentioned. And, like a chronic disease, it needs to be treated for life. That treat for life part I agree with.
But I have a different approach. Watch the video first, then we’ll discuss. The talk is being given to a medical audience, so it is fairly technical throughout. Watch the whole thing if you like, but for purposes of our discussion after, simply start at 9:35 and watch for a minute or two, then go to 30:58 and pick it up for another couple of minutes. I’ve got it queued to the 9:35 point, but feel free to watch the entire video. The video is about 58 minutes long, but the lecture part ends at about 42 minutes. The rest is a Q&A.
After watching a few minutes, go to 30:58.
Here is the medication chart and dietary history of her patient.
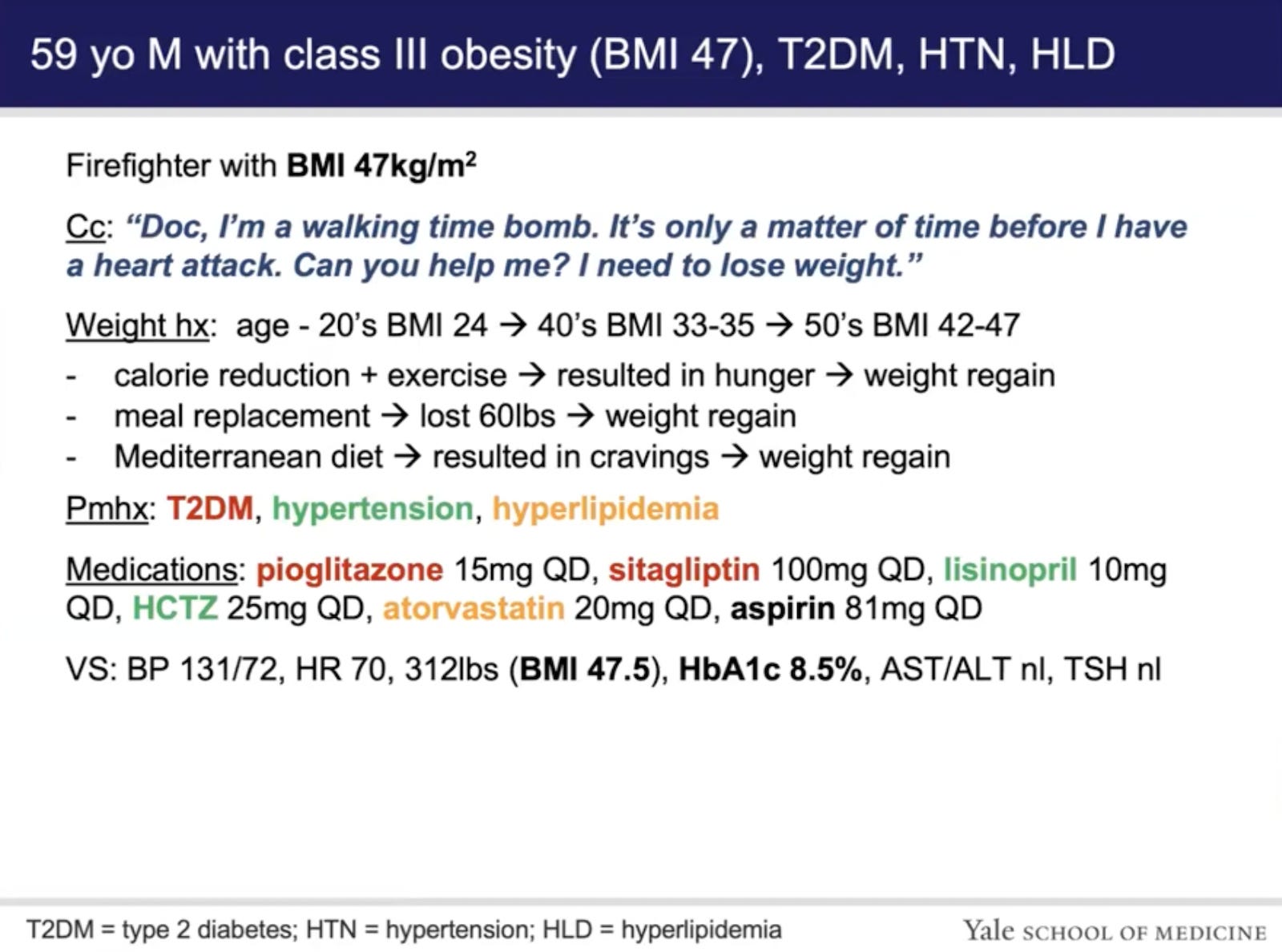
The patient is on the following medications:
pioglitazone (Actos) is a thiazolidinedione, which basically acts to improve insulin sensitivity. (Can sometimes increase weight gain.)
sitagliptin (Januvia) is a DPP-4 inhibitor, which increases the activity of GLP-1. (DDP-4 is an enzyme that breaks down GLP-1. When DDP-4 is inhibited, naturally produced GLP-1 hangs around longer.)
lisinopril (Zestril) is an ACE inhibitor used for hypertension.
HCTZ is hydrochlorothiazide, a diuretic, also used for hypertension. It’s a drug that’s been in use forever.
atorvastatin (Lipitor) is a statin. (Sometimes causes T2DM.)
aspirin in this case is a baby aspirin.
I don’t know this patient’s total medical history, but I can tell you I’ve treated countless patients just like him. I have a different approach than the doc in the video. Her approach is the one most mainstream docs would follow. No one would bat an eye at what she proposes. Which is to put this guy on Ozempic, Wegovy, or Mounjaro. Probably Mounjaro, since she was deeply involved in its study. And she would keep him on it for life. Or until it gets yanked from the market because of side effects.
I would have a long talk with this patient. I would tell him that all of his problems stemmed from insulin resistance. I would tell him the proof of this is that fact that he lost significant amounts of weight using meal replacements, which lower insulin levels fairly quickly. I would explain to him how every symptom he has—obesity, high blood pressure, diabetes, and hyperlipidemia—stems from his insulin resistance and hyperinsulinemia. He has been treating his symptoms with drugs, while ignoring the underlying problem.
I would question him in detail about any side effects he might be having from any of the meds he is taking. I’m sure there would be a few. I would ask him all kinds of questions about his diet and lifestyle. I would ask him about what kinds of foods he likes and what kinds of foods he doesn’t like.
Over the years, I’ve noticed a couple of things about overweight patients. First, many of them have a fairly limited palate. And most of the foods they don’t like are the ones that they should be eating and vice versa. Which makes it difficult for them. If you don’t like meat, eggs, cheese, and other low-carb foods, it makes it tough —though not impossible— to go on a low-carb diet.
Some overweight patients—especially men—like everything. They are the easier ones to deal with. I suspect our patient above falls into this category.
Since most of his issues, at least as described in his history, involve cravings, a low-carb diet should help, because he can always eat. Maybe not everything he’d like to eat, but he can always eat; he needn’t fight hunger.
I would tell him my approach would be to get him off of as many drugs as possible as quickly as possible. And I would point out that he has total and complete control over everything that goes in his mouth. Strange as this sounds, many people take that as an epiphany.
It’s a general truth that most people agonize about things over which they have absolutely no control while giving up control of things over which they have total control. I’m not trying to be a hard ass about it, it’s simply true. Most of us—myself included—spend far too much time stressing over things that are out of our control and give up on things we can control.
No one holds a gun to our heads and forces us to eat. That is one thing we can control completely. And with a low-carb diet, we can always eat if we’re hungry.
I would recommend this patient get a continuous glucose monitor (CGM) and watch it to see how various foods affect his blood sugar. One of the remarkable things I found when I’ve worn one was that certain foods I would have expected to shoot my sugar to the stratosphere did not do so. And other foods I figured were pretty safe ran my sugar up and kept it there. An example of one of the former for me was potatoes. Which kind of sucked because I’m not a great fan of potatoes. One that ran both my and MD’s sugars through the roof and kept them there for several hours was steel-cut oatmeal. Neither of us has ever had it since. Glucose levels, of course, aren’t the only issue. It very well could be that my insulin is still going high with the potatoes to keep my glucose normal, but until they develop a handy dandy CGIM (continuous glucose AND insulin monitor) we’ll not know.
I would tell this man he obviously has a carb sensitivity and hyperinsulinemia, and that he can deal with it two ways. He can either go through the rest of his life popping pills and eating whatever he wants and reap minimal success. Or he can go on a low-carb, ketogenic diet and solve his problem. The first option is easy, but will doubtless cut years from his life. How many, I couldn’t say. The second option will restore his health, but will require some effort.
Based on my experience in having this talk with many patients, I suspect he would be willing to give a whole-food, low-carb, ketogenic diet a try. We would work with him to come up with a palatable diet he could live with that would do the trick. As part of the program, we would tell him how important it is to avoid seed oils, which I think are a big problem with the looming obesity epidemic.
And to avoid highly-processed foods. I’m not just saying this because it sounds like a good thing to say. Processed foods have their structural integrity violated by all the mechanical work done on them. When this happens, these products stimulate the secretion of GIP (glucose-dependent insulinotropic polypeptide), an incretin, which greatly provokes insulin release. The same foods in the pre-processed state might cause some insulin release, but nowhere close to what processed foods do.
Not only that, but GIP also acts to decrease the clearance of insulin, so highly processed foods are a doubly whammy.
I would tell him the day after he starts the diet he should go off his pioglitazone and sitagliptin, the two blood sugar medications, checking glucose with the CGM or a finger stick method. I would tell him to stop the HCTZ the day he starts his diet. I would leave him on the lisinopril at the outset. ACE inhibitors are one of the few drugs I actually like, but it will likely not be needed in time.
And, of course, I would take him off the statin.
So, he would be down to two drugs (assuming you call the baby aspirin a drug) within a day after starting his new diet.
I’ve learned from bitter experience that folks starting on a low-carb diet drop their insulin and blood sugar levels quickly. In fact, it is almost unbelievable how quickly they do so. I tell other docs, who have never put patients on low-carb diets, that they won’t believe what a powerful therapy it is.
The vast majority of patients will drop their sugar levels quickly and reduce their blood pressure right at the outset. They’ll lose a bunch of fluid via urination, so the diuretic is not needed. In fact it would likely put them on their face from low blood pressure if they were to continue it.
I would have my nurse call this patient in a couple of days to see how he is doing. And I would have him email me his CGM readings. Based on past experience, I suspect his sugars would have fallen. I would have him come back in a week for a recheck and debrief. I suspect his blood pressure would be what it was while he was on both meds or even lower. About 75-80 percent of patients can go off their BP meds fairly quickly after starting a low-carb diet. The other 20-25 percent end up having to stay on some sort of medication because hyperinsulinemia and insulin resistance aren’t the only causes of hypertension. If needed, ACE inhibitors are my favorite.
I would recheck his blood values in six weeks, and I’m fairly certain his triglycerides would have fallen like a rock, his HDL would have gone up, and his LDL probably gone down, even after having gone off the statin. Statins work by inhibiting an enzyme called HMG CoA reductase, which is the rate limiting step in the cholesterol synthesis pathway. Insulin stimulates this enzyme and glucagon inhibits it. People on low-carb diets lower their insulin levels and increase their glucagon levels, which regulates the enzyme nicely without all the side effects of a statin.
If you don’t believe how quickly a low-carb diet can reduce and stabilize blood sugar, take a look at the two CGM readings below. Note that the second one is the week after the first one. The patient had the same HgA1c as does the patient in the video lecture we’re discussing. And that’s after God only knows how long on glucose-lowering meds.
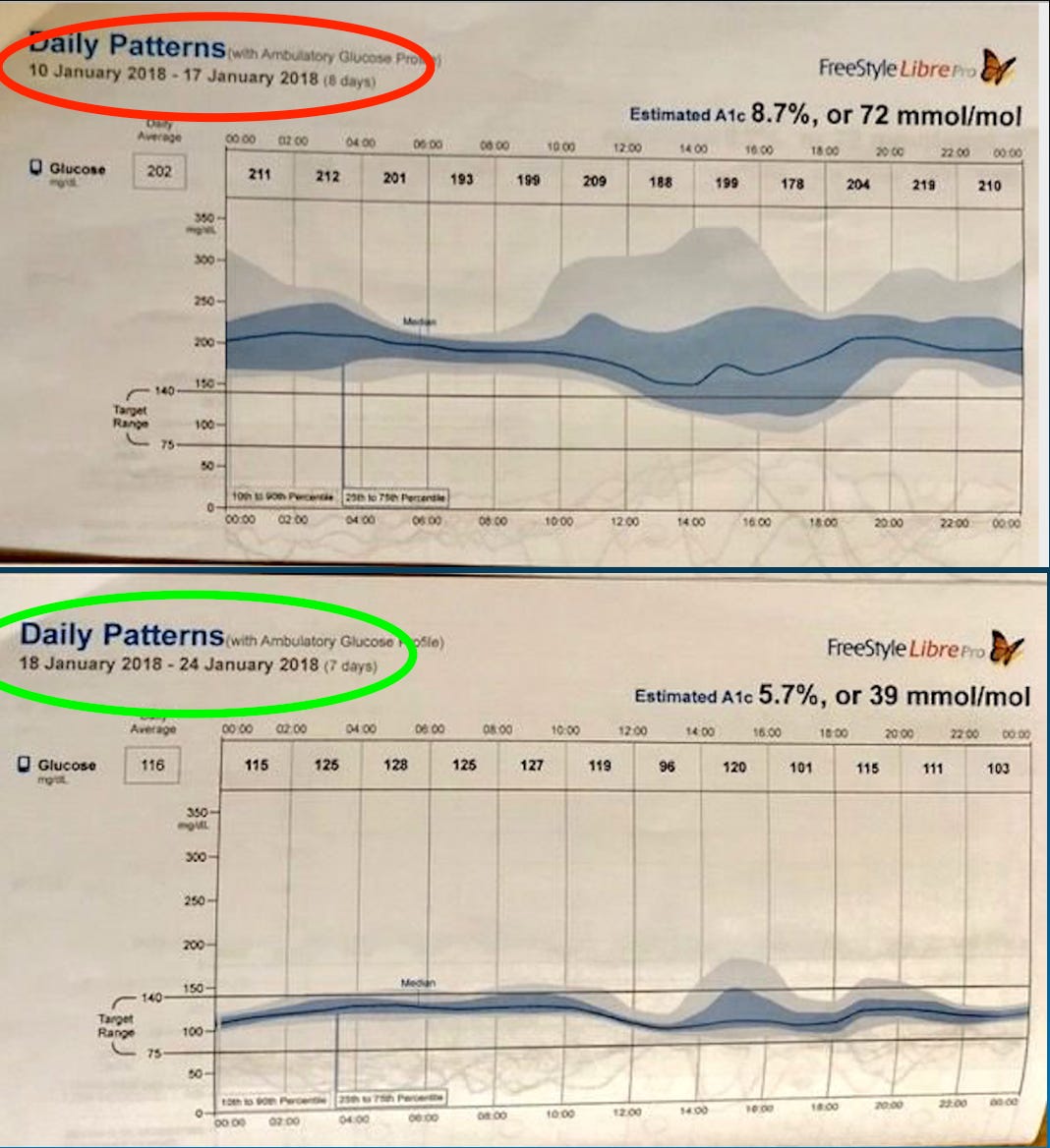
One week! Which is why I don’t worry about removing patients from their glucose-lowering drugs.
During the course of his weight loss, we would monitor him closely. He would have a 75-80 percent chance of coming off his remaining BP med. And we would work with him through maintenance, which is the real danger zone.
I believe he would lose his weight and be medication free. And probably live a lot longer, happier life… as long as he embraced a low-carb/keto way of eating for life. Obesity is a chronic disease, as the Yale doc said in her lecture, and it needs to be treated for life. On that we do agree. But it needs to be treated for life…with a nutritional regimen that keeps all of his symptoms at bay. For most people in his situation, that is some form of low-carb diet.
I suspect most mainstream physicians would prefer the Yale doc’s treatment protocol more than they would mine. And maybe a lot of patients would, too. But I think mine is much better, more effective, and less expensive for the patient in the long run.
Before we leave this section, take a look at the disclosure statement at the start of the Yale doc’s lecture.

You can draw your own conclusions.
Alzheimer’s, Vaccines, and Adherence
Medical News Today just posted an article with the link-bait-y title Routine vaccinations linked with lower Alzheimer's risk. Who could resist taking a look? I certainly couldn’t.
The article is a commentary on a recent study showing an association between the taking of a number of routine vaccines and lower rates of Alzheimer’s disease.
Medical News Today summarizes the findings in the study as follows:
Recent research from UTHealth Houston suggests that the administration of some vaccinations, including those for tetanus, diphtheria, pertussis (whooping cough), shingles (herpes zoster), and pneumococcus, are associated with a reduced risk of developing Alzheimer’s disease.
Previous research revealed that individuals who had received at least one influenza vaccine had a 40% lower probability of developing Alzheimer’s disease compared to those who had not received any vaccination, leading researchers to investigate other vaccines.
These new findings are particularly notable as they point to a practical and accessible way for Alzheimer’s prevention, emphasizing the advantages of routine adult vaccinations.
One of the authors of the study opines.
Kristofer Harris, co-first author on the study and program manager in the Department of Neurology with McGovern Medical School at UTHealth Houston, spoke to Medical News Today, saying the team “found that there is a decreased risk of Alzheimer’s disease for older adults who received routine vaccinations.”
“The risk of Alzheimer’s disease was reduced by 30% with Tdap/Td vaccination, 25% with shingles vaccination, and 27% with pneumococcal vaccination when we compared to those who did not receive those respective vaccinations,” he noted.
Then there was this pull quote about the findings in a previous study the group had done.
“This study goes hand in hand with our previous research, which found that people who received at least one flu vaccine were 40% less likely to develop Alzheimer’s disease when compared with those who were not vaccinated.”
The MND article goes on to speculate how the vaccines might work to prevent Alzheimer’s.
It could be that vaccines change how the immune system acts when there are harmful proteins building up in the brain, a process linked to the development of Alzheimer’s disease.
They might also help immune cells work better in cleaning up these harmful proteins or they could improve the immune response, helping to protect healthy brain cells nearby. [Bold in the original.]
And then the line I had been waiting for.
The findings from the study contribute positively to both Alzheimer’s disease prevention research and public health overall, underscoring the importance of vaccination.
The implication all along here is that routine vaccination somehow wards off Alzheimer’s, when the reality is that it is simply an association. A correlation. And, as we all know, correlation does not imply causation.
The only way you could ever legitimately say vaccines prevent Alzheimer’s would be to do a randomized, double-blind, placebo-controlled study in which a large number of adults are given vaccines while an equal number of age, sex, and health cross-matched adults are given a shot of saline. Then wait around to see what happens. If significantly fewer people in the vaccinated group come down with Alzheimer’s as compared to the unvaccinated group, then you might be on to something.
In case you were wondering that will never happen. Many people have been begging for vaccinated vs unvaccinated studies in children, who are given dozens of shots. No one will do the studies because it would be deemed unethical to not vaccinate the control group. I have no way of knowing for sure, but I suspect the results of such a properly performed study would end up showing it would be unethical to give kids all those vaccines. But we don’t know, because the studies haven’t been done.
One of the physicians MNT reached out to for commentary opined:
Dr. David Merrill, geriatric psychiatrist and director of the Pacific Neuroscience Institute’s Pacific Brain Health Center in Santa Monica, CA, not involved in the study, said that “these findings are consistent with prior work showing that getting the flu shot also lowers risk of developing [Alzheimer’s disease].”
“Now that three additional vaccines have been shown to have this effect, it suggests that perhaps vaccines are working through some additional shared immune-system mediated mechanism to reduce risk of [Alzheimer’s disease],” he added. [Link in original.]
He then goes on to suggest
“…older adults who get vaccinations may also be more likely to take care of themselves in general.”
If there is any connection between vaccines and Alzheimer’s, I would guess it is this one. Not trying to come up with some way to show the immune system, primed by vaccines, can prevent the disorder.
Almost 43 years ago an enlightening article appeared in the New England Journal of Medicine titled Influence of Adherence to Treatment and Response of Cholesterol on Mortality in the Coronary Drug Project.
The article was about a study on clofibrate, a pre-statin cholesterol lowering drug. Researchers wanted to see if the drug might improve all-cause mortality. After the subjects were on either the drug or the placebo for five years, researchers calculated the mortality from the number of deaths in each group. As it turned out, 20.0 percent of those on clofibrate died during the five-year period while 20.1 percent of those on placebo died. So, essentially no difference. Clofibrate, despite lowering cholesterol levels, did not decrease all-cause mortality any more so than taking a placebo.
The researchers dug a little deeper into the data and discovered that only 15.0 percent of those subjects who took 80 percent or more of their clofibrate doses died. And of those who took it sporadically, 24.6 percent died.
So, in the end, a big win for clofibrate and its cholesterol-lowering properties, right?
Not so fast.
When the researchers dug even deeper, they found that only 15.1 percent of those subjects on the placebo arm who took their pills at least 80 percent of the time died. The same as clofibrate.
And of those who took their placebo sporadically, 28.3 percent died.
So it wasn’t a win for clofibrate and cholesterol lowering. But it was a win for science. The scientists involved realized that people who adhered to instructions were a different breed of cat, so to speak, than those who didn’t.
They called this the adherer effect. And it has been studied many, many times. Adherers always do better than non-adherers in both the study arm and the placebo arm.
Often researchers publishing observational studies ignore the adherer effect, because not ignoring it might make their study look inconsequential.
Years ago when statins were being studied right and left, I remember one that was hailed as proof that statins worked. I can’t remember the name of the study at this point—I’m sure I have it in my files—but I remember what I thought when I read it. Two words. One starts with B, the other with S.
Here’s how it worked. A lot of observational studies are done like this, so beware.
Doctors put patients with elevated cholesterol on a particular statin. The docs gave the patients a chit for them to get their statins free every month. At the end of whatever this study period was—several years, as I recall—they looked at how many chits had been turned it and compared the outcomes between those who got all their statin prescriptions filled and those who didn’t. Or who got them sporadically.
Of course, significantly fewer of those who got them like clockwork died (or suffered heart attacks—I can’t remember the end point) as compared to those who didn’t.
The authors of the study proclaimed the life-saving (or heart attack preventing) virtues of the statins involved, when it was doubtless the adherer effect they were seeing.
I strongly suspect it is the adherer effect kicking in on the routine vaccination-Alzheimer’s situation. Since vaccines have such a halo effect, most people who are serious about their health—adherers—will get every vaccine that comes along. These are the same people who watch their diet, exercise more, and, in general, live a more healthful lifestyle.
We won’t know for sure unless there is an RCT, which means we won’t ever know for sure, because there won’t ever be an RCT looking at this.
But it is what I would bet on.
Is Seed Oil Bashing a Right Wing Conspiracy?
Rolling Stone magazine seems to think so.
I was flipping through Rolling Stone online a couple of days ago and came across an article headlined Why Is the Right So Obsessed with Seed Oils? The article itself is idiotic. It goes through and talks about a few people who may or may not be far right who believe seed oils are killing us.
Here is a sample.
In truth, while Carnivore Aurelius’s posts are perhaps exemplary of slightly more intense anti-seed oil rhetoric, the vitriol is pretty much everywhere. All over Instagram and TikTok, wellness influencers are urging their audiences to avoid buying products with seed oils in them, to the degree that there are more than 126 million views under the #seedoils hashtag on the latter platform. It’s particularly common among right-wing or right-wing-adjacent circles, where the fear over seed oils has almost achieved meme status: “Left wing hypochondria is Covid. Right wing form is seed oils, touching a grocery store receipt, artificial sweeteners, and on and on,” right-wing influencer Mike Cernovich tweeted earlier this month. [Links in original.][My bold emphasis.]
The only substantive argument for why seed oils are good is found a few paragraphs down.
For years, seed oils have frequently been used in cooking and in processed foods because they’ve traditionally been thought of as a healthier alternative to butter, says Guy Crosby, adjunct associate professor at the Harvard T.H. Chan School of Public Health. “Butter is very high in saturated fat and oils are much higher in unsaturated fat,” he explains. “So they tend to be more healthy in terms of [preventing] things like potential heart disease.” [My bold emphasis]
I suspect most of you know what I think of this. And the first word starts with B…
It’s not only bad science, it’s bad grammar. Healthy means a state of being. I am healthy. You are healthy. He, she, and it are healthy. You know the drill.
Unfortunately, many people use the word “healthy” when the word they want to use is “healthful,” which means promoting good health. You eat healthful foods to make you healthy. Foods are not healthy. Unless they are alive and growing splendidly. Then you could say, Wow, that’s a healthy looking bunch of corn or apples or whatever.
Drives me nuts.
If I had to make a call as to why this article was published, it might be that various seed oil companies advertise on Rolling Stone. Mainly lefties read Rolling Stone (I’m an exception), and I suspect the article is aimed at them. I would bet as many lefties as righties are anti-seed oil. But if there is one thing a lefty can’t stand, it is doing something thought to be right wing. Which means the majority of readers of Rolling Stone who do think seed oils are bad might give it up if continuing to think that way meant they could be associated with the right.
Any way you want to cut it, the article is moron-level persuasion.
When you look at what has happened to the food supply since the obesity epidemic started, the only food product category that has significantly changed is seed oils.
Here is a slide from a talk I gave a few years ago demonstrating just how much it has changed.
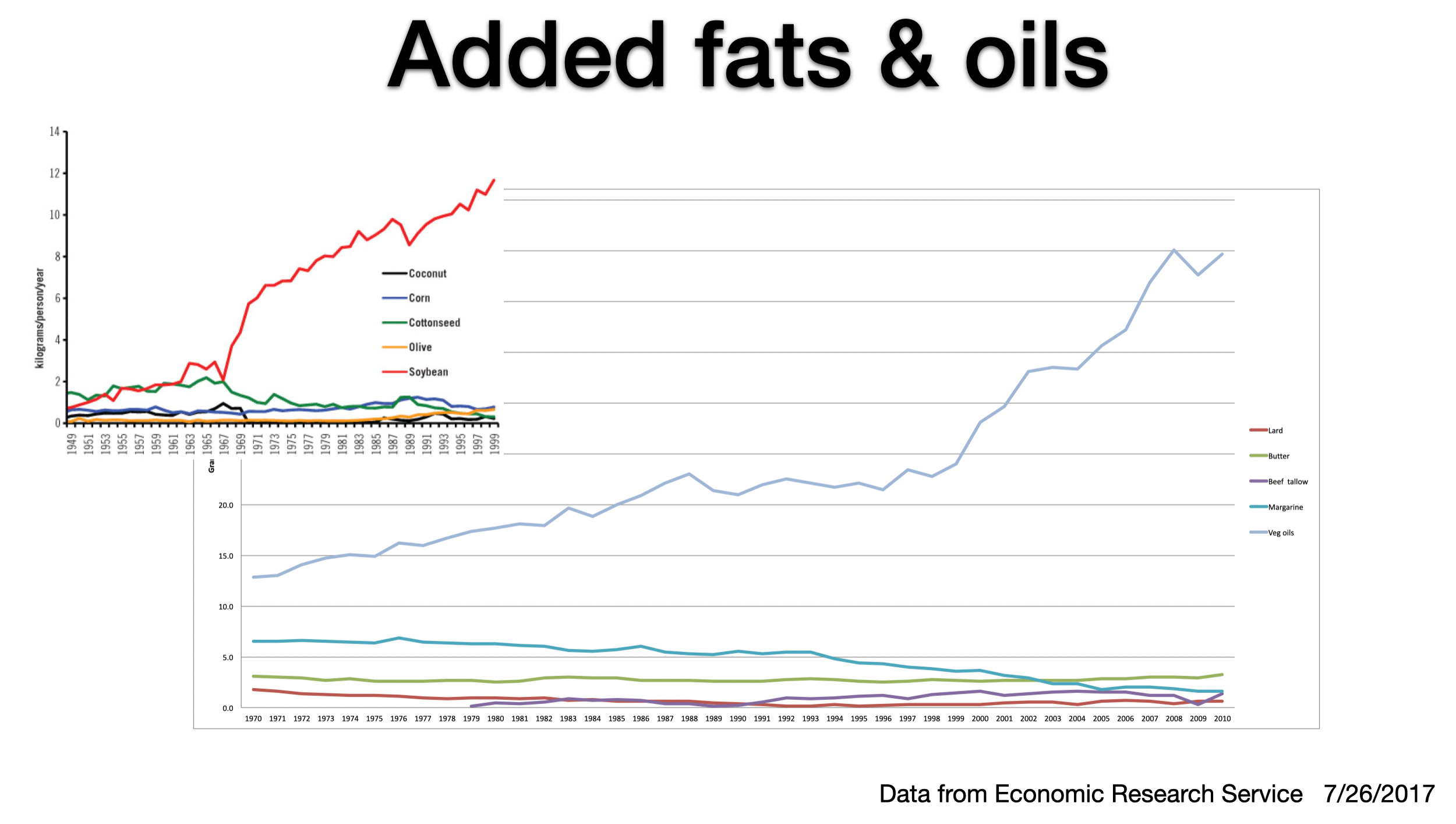
It’s a bit difficult to see, but the big chart shows how we have decreased consumption of all kinds of other fats while vegetable (seed) oils consumption (the blue line) has skyrocketed. The smaller chart at the upper left shows that soy bean oil is the main seed oil we’ve all been eating. And soy bean oil is loaded with linoleic acid, an omega-6 fat.
Here’s another.
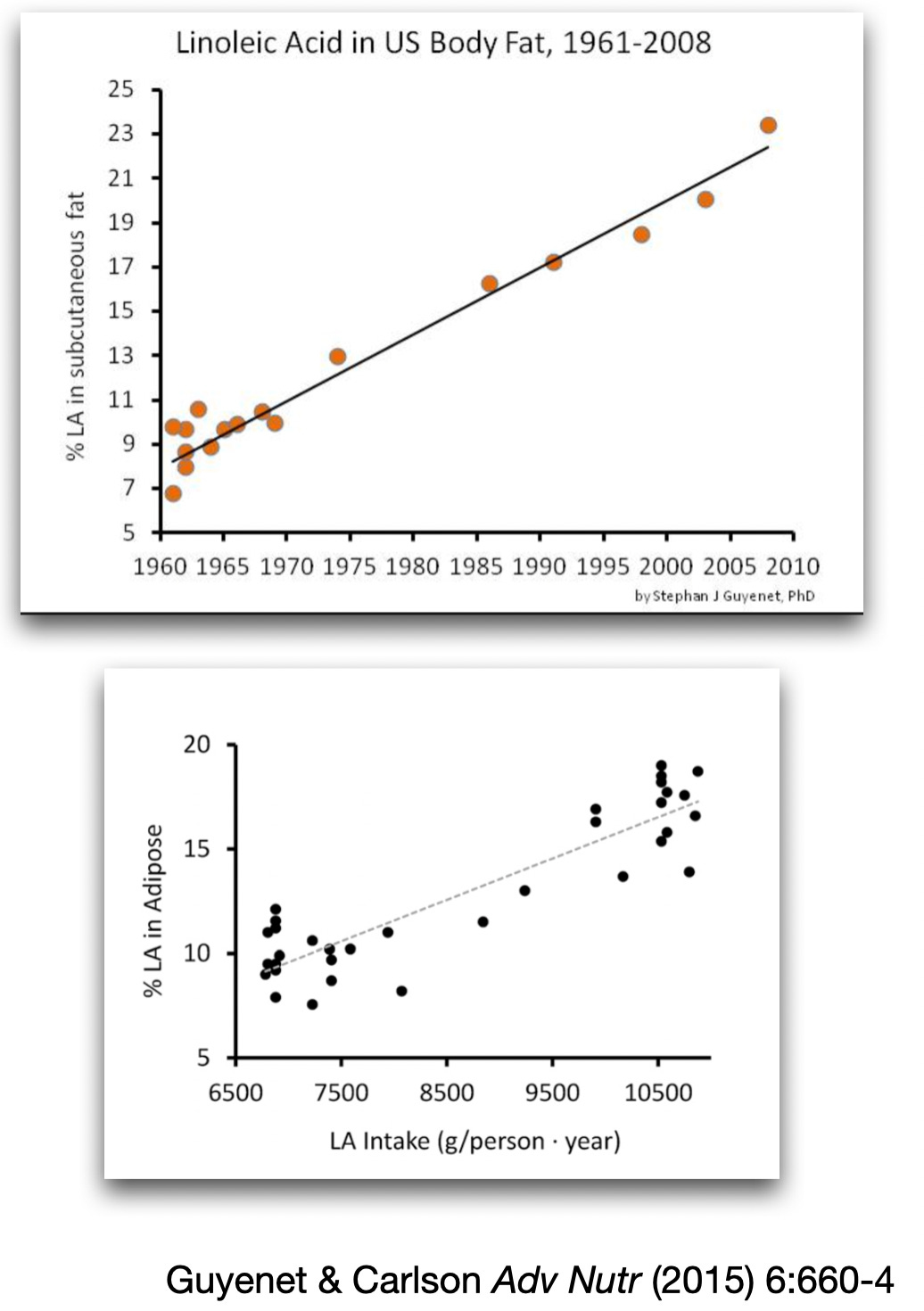
These charts show the increase in linoleic acid consumption (top chart) and the increase in human tissue linoleic acid as a function of the amount consumed.
There are a half dozen theories as to why linoleic acid and other polyunsaturates are not good for us. I laid out the hypothesis I think is most valid in a talk I gave several years ago. Nothing since has changed my mind.
You can watch the talk here, but be forewarned, parts of it are fairly technical.
Okay, on to the VOTW
Video of the Week
In a previous Arrow I wrote about how I ran with (from?) the bulls in Pamplona, Spain when I was in college. I had told the story to our kids countless times, so when the youngest graduated from college and we asked where he wanted to go (we had taken both his older brothers on nice trips to celebrate not having to pay private school tuition), he said Pamplona to run with the bulls.
So he and MD and I went to Pamplona, and we all ran with the bulls.
One of my favorite books (and a mini-series on TV) is Lonesome Dove. There is a great scene in both the book and the series in which Gus, the main character, wants to go out and chase some buffalo. Pea-Eye, one of the supporting characters, doesn’t want to have any part of it. When Gus asks him why, he says, “Them bulls’ll hook you.” (You can see the scene here—it’s brilliant. And right out of the book.)
When MD and I and youngest kid were in Pamplona getting ready to run, Them bulls’ll hook you was much on everyone’s mind. Fortunately, none of us got hooked. But the same can’t be said for the poor guy below.
When we ran, we noticed that the bulls just kind of plowed through the crowd, but once in a while, one would get pissed and single out one individual for retribution. The guy below got singled out. Could have been bad, but he seems to have come out of it okay.
Okay, that’s about it for today. Keep in good cheer, and I’ll be back next Thursday.
I almost forgot the poll.
Thanks for reading all the way to the end. If you got something out of it, please consider becoming a paid subscriber. I would really appreciate it.
Finally, don’t forget to take a look at what our kind sponsors have to offer. Dry Farm Wines, HLTH Code, Precision Health Reports,and The Hustle (free).
A bit off-topic, but related. Watched the Netflix docudrama "PainKiller," the other day (6 episode limited series), about Oxicontin. If even a 4th of the dramatization is accurate, then wow, and it takes no effort whatsoever to understand the disaster that is the covid drug trials.
In my view, the entire system is as corrupt as it's possible to be and one wonders whether you could do better when in need with street drugs from reputable dealers who take their interest in long-term customer longevity seriously.
It’s a shame because if you don’t want to take pills, it’s really hard to find any healthcare or even get good advice. 95% of doctors just give you a pill. Depressed, overweight, or acid indigestion…answers are all the same….