




Hello everyone.
Greetings from a wet and dreary Montecito.
I’m cranking out this 115th edition of The Arrow earlier in the week than usual, so if I miss covering something of tremendous importance that occurs later in the week, you’ll understand why. We’ve been on flood watch here since 8 am Tuesday morning (which is when I’m typing these words). There are mandatory evacuations in place for large portions of Montecito, but, fortunately, not our specific location. But that could change quickly. As a precaution, all the schools are closed. It has been raining relentlessly all night long and hasn’t let up. But it’s not a hard rain, just a constant one, a type of rain the Navajo call a female rain.
Just a couple of months ago—while we were in Dallas—there were huge rains that flooded much of Montecito, but this time, thankfully, with no loss of life. Such was not the case five years ago when a sudden rainstorm created a huge mud and debris slide that killed 23 people here, including a couple of our neighbors. It was a freak occurrence in that the heavy rain (which had been missing for years because we had been through a major drought) came on the heels of the Thomas fire, the largest fire in California history at that time, that burned from Ventura through the hills right above Montecito.
The fire had burned all the vegetation, which was incredibly dry due to the years long drought, and when the sudden intense rainstorm—definitely not a female rain—hit the bare ground that had been baked to glass by the fire, water flew down all the little streams—normally dry as a bone—carrying a river of heavy, thick mud and huge boulders along with it that crashed through homes and destroyed pretty much everything in its wake.
Just to give you an idea how bad it was, below is a photo of the street running right by our house after the clean up had been underway for a couple of months.

The road you just barely see turning off to the right in the foreground was where we lived when we were in Montecito. Had you turned up that street, our house was the first one on the right.
Here is what it looked like early on the morning of Jan 9, 2018.

The roof you see on the right between the two big trees was from a house destroyed by the debris flow. Two people who were there died; one was in the giant debris pile you see in the mid-distance. Here it is in a closer view.

Note the size of the boulders that crashed down on everyone. The mixture of the rain water, the mud, and the ash from the fire created a kind of concrete-like mix that picked up and floated enormous boulders for hundreds and hundreds of yards.
MD and I were in the wrong place at the wrong time. We had come down from our home in Tahoe for a get together with friends in early December down in Malibu. The night before the get together, the Thomas fire hit Ventura. We drove through all that to get to Malibu. Had our get together, spent the night, and drove back to Montecito. Our plan was to spend the rest of December in Montecito and have Christmas with the kids there.
As it turned out, we were evacuated for almost two weeks due to the fire. We—son, and 2 dogs—decamped to a hotel in LA. Our DIL and two grandkids had already headed south to escape the smoke. We all stayed first in LA, then when it looked like we were going to be evacuated for an indeterminate time, decamped to a VRBO in the desert. We ended up being allowed back into Montecito on Dec. 23, which allowed us to be there for Christmas. Since we had been displaced so long because of the fire, we decided to stay a little longer. Then the debris flow hit in the early morning hours of Jan 9. The road pictured above was the only way out going one way. About a half mile the other way the road was washed out and buried, too. So we were trapped for three days. Without utilities.
Finally, a narrow part of the road pictured above was cleared, and the Santa Barbara County Sheriff’s team were able to help us drive out. As you might imagine, we kept on driving the nine hours back to Tahoe and stayed there.
Others fared vastly worse than we did. The events of that night are still seared deep in the minds of everyone who was in Montecito at the time. We were lucky as we had our home up north to go back to. Others not so much. They had to range far and wide to find accommodations as the area was closed for almost a month while workers toiled round the clock to remove thousands of tons of debris and cadaver dogs searched for bodies, one of which has still never been found.
Since we’ve all imbibed the tragedy of Jan 9, 2018 deep into our consciousness, we all know what can happen. So whenever there is a constant rain like the one we’re experiencing now, everyone casts a frightful eye at all the rushing streams coming down off the mountains. And worries. So far, thankfully, so good.
Okay, when I set out to write this week’s Arrow, my intention was to avoid anything having to do with Covid, but there is so much happening this week, I just can’t let it slide. Mostly, though, it involves political chicanery and how we’ve all been lied to repeatedly, so it’s not so much about Covid itself, but the political reaction to it.
First, let’s revisit the mask brouhaha.
Masks…Again?
Just when you thought it was safe to go back into the water…
As I wrote about recently, the Cochrane collaboration published a report analyzing the available data and declaring there isn’t any body of evidence showing masks are protective against the influenza and Covid viruses. I figured that would be the end of it. But I hadn’t counted on the seductiveness of masks to a large segment of the population. It’s almost as if the lust to mask is a part of their DNA.
Perhaps it’s the only visible thing these folks can do to ‘prove’ they really are better than the rest of us. That they do care more. That they follow “The Science.” Whatever the reason, the Cochrane paper brought them out in force.
The mass of these folks went wild, but that wasn’t enough to cause a direct effect. Then Columbia University journalism professor Zeynep Tufekci wrote an opinion piece for the NY Times breathlessly titled “Here’s Why the Science Is Clear That Masks Work,” which provoked a statement from the Cochrane group clarifying its statement, the essence of which is shown below.

Let me show you just how stupid this is.
When researchers study the effectiveness of an experimental drug, they provide the drug and a placebo that looks exactly the same to the subjects, who have been randomized into either the study group or the control (placebo) group. They send these subjects home with instructions on how to take the drug: once per day, twice, three times per day, whatever. So the subjects go home and take them as instructed. Or don’t. There is never complete compliance.
The usual way compliance is monitored is by seeing if the subjects pick up their pills when they’re supposed to. And by having them return any pills they didn’t take. Now let me ask you a question. If you were in a study you were getting paid to be in, and you were supposed to take a pill every day, and you discovered at the end of the month when you were supposed to come in for your refill that you had taken only 12 of the 30 given to you, would you bring the other 18 in and fess up that you hadn’t taken them? Most people wouldn’t.
This is how drug studies are conducted. They don’t bring the subjects in daily or twice a day or, God forbid, three times a day and witness them taking their pills. They rely on the subjects to be compliant.
Yet when the results come in and all the codes are broken to see who was on the study drug and who was on the placebo, if the study drug shows a significant change in whatever parameter was being studied, then it is reported as a success. Or if it doesn’t show a difference, it’s reported as a failure. At least today with the new reporting laws. In the past, it just wasn’t reported.
So, in accordance with what the Cochrane statement above says, what these drug reports should really say is not that the drug was effective, but that
”interventions to promote” the regular use of the study drug were effective. Or, if the drug were not shown to be effective, then “ it would be accurate to say that the [study] examined whether interventions to promote [regular use of the study drug] helped to [treat whatever the study drug was meant to treat], and that the results were inconclusive.”
This is of course insane. No one would publish a study with those results. It was the drug being studied, not the “interventions to promote” the drug’s use.
In the mask studies, selection by randomization or other means divided people into two groups. One group was asked to wear masks while the other was asked not to. There was no significant difference in outcome in terms of getting Covid. End of story.
The only way a study can be done to definitively determine the effectiveness of mask wearing would be to put each subject under supervision 24/7. If the masks came off at any time, then that subject was kicked out of the study. If a subject in the unmasked group got worried and put a mask on because she was going into a crowd, then, boom, gone from the study.
I suppose another way, which, of course, would never make it through the Institutional Review Board (that has to approve all studies), would be to find subjects with no antibodies to Covid, mask them, then spray an aerosol containing SARS-CoV-2 into their faces. Do the same with unmasked subjects. If there were a significant difference in numbers who contracted Covid-19, that might prove something.
The fact that the Cochrane report showed no real effectiveness of mask wearing based on data from a large number of studies confirms the point physicist and founder of the Stanford Linear Accelerator Center, Pief Panofsky made when he said "if you throw money at an effect and it doesn't get bigger, that means it's not really there."
If you want to read more about this debacle, take a look at Maryanne Demasi’s substack piece on it along with Paul Thacker’s The Disinformation Chronicle.
But if you want some fun reading, go to the link above to the NY Times article and read the comments. It is confirmation bias write large. Oh, thank you, Professor Tufekci (whose training is in sociology) for telling me what I knew was the truth all along. I’ll continue to wear my mask proudly to show that I’m not ignorant of “The Science.”
Jesus wept.
Vaccine Bombshell
I came across the most devastating critique of the Covid vaccines yet, and I can’t remember where I found it. I’ve sent it to so many people and discussed it so often, that I absolutely cannot recall where I came across it. But I was bowled over when I did.
It is too complex to discuss in detail because it would take up this whole issue of The Arrow, so I’m going to post the video below. You can either watch it or not. It’s basically about how shoddy the entire process of designing and manufacturing the vaccine has been. And it tells me why there is such a variation in batches as reported by howbadismybatch.com.
The woman who narrates the video is a Canadian pharmaceutical researcher and regulator. I couldn’t find a lot of information about her, but she is listed as one of the authors of a group of books on evidence-based drug & therapeutic information for Canadian Healthcare Courses. Which would imply that she is in the mainstream of the Canadian pharmaceutical world.

While she was working from home during the lockdowns, she decided to do a thorough review on the application process for the various Covid-19 vaccines. What she found is truly astonishing. Some of it is fairly complex, but she explains most of it pretty well. And it is devastating.
Obviously, it wouldn’t see the light of day on YouTube, but you can find it on Bitchute.
I look at the stats each week for my content and only four to six percent of people ever click on these video links. This is one you really should take the time to watch just to see how totally slipshod the approval process was for these injections. And how sloppy the manufacturing process, which is also supposed to be regulated.
Major Exposé in the UK
I’ve been eating this one with a spoon. I have a lot of UK readers who write telling me they enjoy The Arrow, but much of my commentary on American politics flies right by them because they don’t fully understand our system. Well, now it’s turn about. This doesn’t have as much to do with the Brit system as it does with the lockdowns in general and how they were ‘masterminded’ in the UK. Probably in much the same way they were here. Run by idiots.
Here is the situation in brief.
Matt Hancock, a British politician, was the Secretary of State for Health and Social Care, which is a cabinet position comparable to the Secretary of the Department of Health and Human Services (HHS) in the United States. In that position he was responsible for much of the damage done to the UK by strict lockdowns and other stupid (in my view) efforts to stem the spread of Covid. One of which in a bit of irony jumped up and bit him in his own hind end.
He had proscribed draconian social distancing rules that were to end on May 17, 2021. In June of that year, The Sun, a Brit tabloid, published a photo of Hancock in a lip lock with one of his advisors (both were married to other people) on May 6, a bit over ten days before the rule was to end. One doubts that was the first time he breached the rule, which disallowed intimate contact between people from different households. He, of course, offered a cringe worthy apology, then, surprisingly, quickly resigned a day later.
The next year it was announced that he was writing a book that would be released at the end of 2022 titled The Pandemic Diaries, which was to be all about how he dealt with the pandemic and the rest of the government players involved. He hired Isabel Oakeshott, a Brit political journalist, to be his ghost writer.
Oakeshott asked for and received all of Hancock’s correspondence on events surrounding the pandemic, including a huge trove of WhatsApp messages (apparently the texting app used by the administration) of his communications with everyone re the pandemic.
She wrote the book, which came out in December of 2022. Then she decided that it was greatly in the public interest to reveal the material in these voluminous WhatsApp messages, which, by her count, represent three times the number of words in the Bible. This she did despite having signed a non-disclosure agreement with Hancock before he turned over all the materials.
I have a bit of an issue here. I am malignantly loyal. I’ll hang in there with someone I’ve come to even a verbal agreement with long past the time I should have gone. So, I’m sure if I were in Isabel Oakeshott’s shoes, I would not have revealed this information.
She turned it over to The Telegraph, the one major conservative paper in the UK. A question remains as to whether she got paid for turning these texts over, and if so, how much was she paid. She terminated an interview with the annoying Cathy Newman over it.
Although I do know a fair amount about the workings of the UK political system, I am unsure as to how much of what goes on that isn’t vital to the nation’s security is made available to the public. In the US, it’s supposed to be pretty much anything. Texts and emails between government officials are all supposedly available here in the US through FOIA. I don’t know about texts, emails, etc., sent via non-government devices that are in reference to the workings of government. I suspect those would be fair game as well.
I don’t know if WhatsApp is the approved UK gov’t means of text communications between officials or not. Nonetheless, they are all about dealing with the pandemic, and in a mass of words greater than three Bibles, they provide insight into the thinking of those involved.
The Telegraph had an entire crew—including Oakeshott—working on them for weeks before releasing them piecemeal in a progression that tells the story. You can read the introductory one here, the first installment showing how, while publicly stating the opposite, Matt Hancock sold nursing homes down the river, and here is a sort of summary of many of them with all the links to the individual stories.
They are all typical of government elitism, double dealing, and incompetence: the mainstays of every government. But what I found more interesting than the revelations themselves is how the press treated Isabel Oakeshott when she revealed this material.
It was exactly how our press treated Matt Taibbi and Michael Shellenberger when they revealed what they had found in the Twitter files about massive government involvement in promoting censorship and what has now turned out to be misinformation (and probably disinformation) about Covid, the lockdowns, and, especially the vaccines. Their fellow journalists turned on them for doing the job that journalists were supposed to do: investigative reporting.
As in the US, the UK journalists, for the most part, were cheering on the lockdowns and not asking any questions. And if they did ask questions, just like their counterparts in the US, they didn’t probe the reasons for the lockdowns, their questions were along the lines of Why didn’t we lockdown sooner? Why didn’t we lockdown harder? Etc. Now that they know how they were hoodwinked by the government, they aren’t pissed at the government, they’re pissed at Isabel Oakeshott, the journalist who proved they were hoodwinked.
I’ve watched a ton of interviews with her—most of them vaguely if not outright—hostile. This one veers that way a bit, but not like a lot of others. In just the first few minutes she describes the treatment she’s received at the hands of her fellow inky wretches (does that description even still apply to journalists any longer?). Well worth a watch.
Okay, on to just a little more Covid-ry, then I’m finished.
The Truth About Ivermectin
Every week I get an email or two or three from people sending me studies showing that ivermectin works against Covid or that it doesn’t. If you look hard enough, you can find a study to tell you what you want to hear. (See above re masking.) But what is the truth in terms of Ivermectin?
Early on I read a few studies and case reports from doctors who had used the drug successfully on Covid patients. And I read some negative studies as well. The sum of the evidence persuaded me that ivermectin probably worked, but more importantly, that it had almost zero downside. It’s the total opposite of vaccinating children. There you have no upside, but major downside potential.
I could’t figure out how our leaders in the CDC and other federal agencies could badmouth such a valuable drug until I realized it stood in the way of their getting the vaccines approved under an Emergency Use Authorization. As we discussed last week, hydroxychloroquine was an approved drug early on, because no one expected the vaccines could be produced as rapidly as they were. Once it became apparent that the actual vaccines could be available soon, they knocked hydroxychloroquine off the list.
The video I’ll link to below mentions that, but just in passing. As I did in an earlier version of this newsletter two years ago, I looked it up again, just to be sure I remembered correctly. And that the video was correct. Here is the link to the entire document. Below is the pertinent section. The highlight is mine.
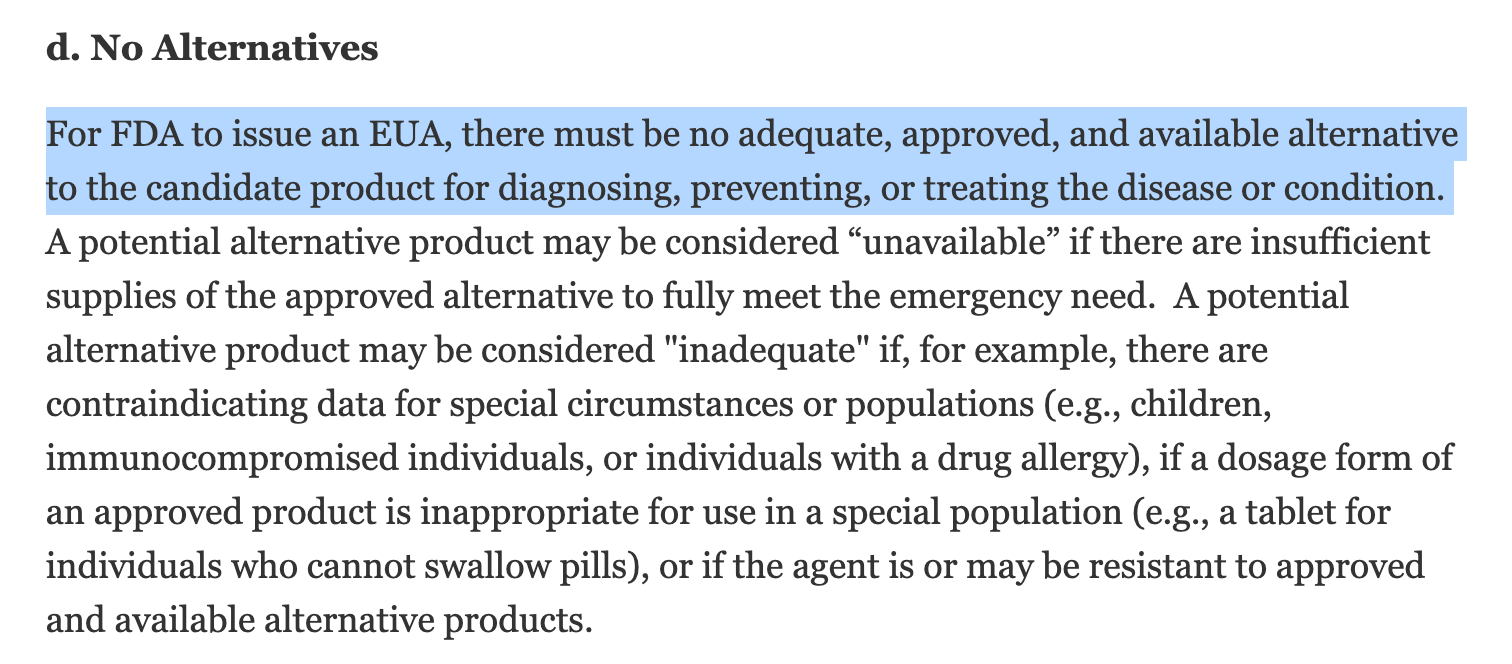
As you can see, ivermectin and/or hydroxychloroquine would have seriously jeopardized getting an EUA. That’s an understatement. Those drugs would have prevented an EUA from being given. And would have put a crimp on the bottom line of Big Pharma since the Covid vaccines have been the biggest money makers in pharmaceutical history.
Talk about regulatory capture. The whole vaccine fiasco shows it in spades. The entire FDA has been captured by the pharmaceutical industry. Approving the bivalent vaccines for infants 6 months and older is a case in point. That was a bridge too far for even Dr. Paul I’ll-vaccinate-anyone-who-will-hold-still Offet to cross.
I don’t know the guy who made this video on ivermectin, but it doesn’t have one false second in it that I could see. I’m glad I came across it, because now I have something I can send to anyone who emails me about an ivermectin study. I just wish more time were spent emphasizing the EUA and how that could not be gotten without throwing ivermectin and any other early treatment medications under the bus. Since ivermectin took the most heat from the press—the segments in the video are disgusting—it was obviously the one most feared by Big Pharma.
It also shows what lapdogs the press are for the government and Big Pharma, which is what so pissed off Isabel Oakeshott when they turned on her for outing their incompetence.
As you might imagine, this video wouldn’t have lasted five minutes on YouTube, so you’ll have to watch it here on Rumble.
And just so you’ll know what a functioning press used to be like, here is a video of Mike Wallace taking a look at the swine flu vaccine, which was ultimately pulled from the market after just a few serious adverse events. Where is this kind of journalism today? James Madison, one of the authors of the Federalist Papers, believed a free and active press was a precondition for self government. Now we’ve got a lapdog press that aids and abets the seats of power instead of investigating and shining a light on the workings of the government.
Okay, enough on Covid-related issues.
Let’s move on to the diet and medical information. And the Video of the Week, which is a good one this week.
But before we get to that, I’ve just gotten notice that I’ve been invited to speak at the LowcarbUSA San Diego meeting, so....
LowcarbUSA San Diego Conference

As you can see, it will all take place in sunny San Diego Aug 17-20.
Here is the specific info for those who might be interested. I just discovered that if you sign up on or before March 31 and use the code MarchMadness, you’ll get a 30 percent discount on the ticket price.
Unless I change my mind, I’ll be giving an update to the mass balance theory of weight gain and loss.
I met a bunch of folks who are Arrow readers at the Boca Raton conference in mid-January of this year. I would love to meet a bunch more in San Diego.
Cancer As a Mitochondrial Metabolic Disease
After last week’s foray into this subject, I’ve been thinking a lot about it. It’s pretty easy to understand cancer if you think about it as a genetic disease. Something goes haywire in the replication process leading to a mutant cell that ends up going wild, replicating like crazy, rapidly accumulating in mass, and finally spreading throughout the body. You can almost see the video in your mind’s eye.
The idea of cancer as a consequence of disorder mitochondrial metabolism is much more difficult to visualize. And even to understand without understanding the underlying science.
So, I’ve decided to break this discussion up into smaller chunks and spread them over a few weeks.
Based on emails I’ve received, I understand I have readers with a wide breadth of scientific training ranging from a lot to none. It’s difficult to explain science in a way that it’s easy to understand by those with little to no scientific training, yet keep it interesting for those who are scientifically trained. I’ll do my best to explain simply without being boring. That’s my goal, at least.
In my view, one of the major difficulties in sorting out the causes of cancer and the best means of treatment arises because unlike any other serious disease, cancer sometimes goes into spontaneous remission. Some cases of cancer, even serious, life-threatening, stage 4 cancers just magically go away. Not many, very few, in fact, but some do just disappear.
Let’s look at a typical example. A man gets diagnosed with a particularly aggressive cancer. He and his oncologist decide to pull out all the stops and do whatever to treat the cancer. Typically, this will have the common trajectory of reduction of the cancer size, then a quick regrowth. When our patient finally exhausts all the therapies available to him, and the cancer gets worse, both he and his oncologist realize the end is near.
A friend of our patient encourages him to go to some sort of psychic healer, who allegedly has had tremendous success treating terminal cancer with beet juice (I’m making all this up—I have no idea if anyone uses beet juice to treat cancer). Our patient, who at this point is literally at death’s door, figures What do I have to lose? So he visits the healer who waves a hand over him, chants, and sells our patient beet juice. Our patient goes home, drinks the beet juice, and doesn’t really notice a change. But day after day, he slowly begins to feel better.
After a couple of months, he feels pretty much like his old self. He goes for a follow up appointment with his oncologist, who is amazed at his appearance. He looks normal. He tells his cancer doc that he feels fine. The doc decides to do a scan, and lo and behold, the man’s cancer is gone.
Our patient’s cancer has undergone a spontaneous remission.
Given this scenario, do you think our patient would be a believer in beet juice as a viable cancer therapy? You bet he would.
And that’s the problem. The real fly in the ointment, so to speak, in cancer therapy. Even though spontaneous remissions are rare, there are enough of them out there to muddy the waters of cancer therapy.
Way back in my engineering days, I read a book by a doctor named William A. Nolen titled The Making of a Surgeon, which was about his time in his surgery residency. It was one of the motivators for me to go to medical school and, ultimately, train in surgery. Once Dr. Nolen went into practice, he started writing other books on various aspects of medicine. And I read them all. He wrote one titled Healing: a doctor in search of a miracle, which was about his travels throughout the world investigating psychic surgeons and a wide variety of non-traditional healers of one kind or another. Since he knew what he was looking for, he was able to debunk all of them as the shams they were.
At the time, Kathryn Kuhlman, a famous faith healer, was filling giant stadiums with people coming to hear her and to be healed. He went to one of her events in Minneapolis, which was near where he practiced, and ended up—as I recall—being able to talk to her in person. And get a list of about 25 people in Minneapolis who had allegedly been healed of various maladies as a consequence of being present at one of her healing services. He tracked them all down and discovered that not a one of them had actually been healed.
But he did make a point in the book that has always stuck with me. He said that in his many years of practice he had taken care of maybe 5,000 patients with cancer (I’m guessing at these numbers, because I don’t have the book in front of me, so am going by memory) and of those patients maybe there had been two or three who had experienced spontaneous remissions. He then wrote that Kathryn Kuhlman probably saw that many cancer “patients” in a week at her many enormous services. So it should be expected that a handful of them would experience spontaneous remissions, and would all attribute it to Kathryn Kulman.
It would be difficult not to.
Here is a nice link with some references if you want to read more about spontaneous remission.
We’ve all had “spontaneous remissions” from influenza, measles, chicken pox, various cold viruses, and even Covid. Had we not, we would be dead. These spontaneous remissions come about because our immune systems, which at first were overcome, were ultimately able to defeat the virus or bacteria that caused the problem.
We are generating mutating cells like crazy all the time, but our immune system recognizes them as foreign—just like it would a virus—and proceeds to wipe them out. Occasionally some seem to make it through and take root, but it’s a difficult process. I didn’t realize just how difficult till I read Jason Fung’s The Cancer Code, which I never get tired of recommending because it is so informative.
I suspect these spontaneous regressions occur when the immune system re-recognizes the cancer cells as foreign and starts rooting them out. The whole idea of immuno-therapy for cancer is based on this idea. Sometimes it works fabulously well; other times not at all.
So, with that all said, let’s dive in and start laying the foundation for the mitochondrial metabolic basis of cancer.
First, I want to put up the same graphic I did last week, but explain it a little better this time.
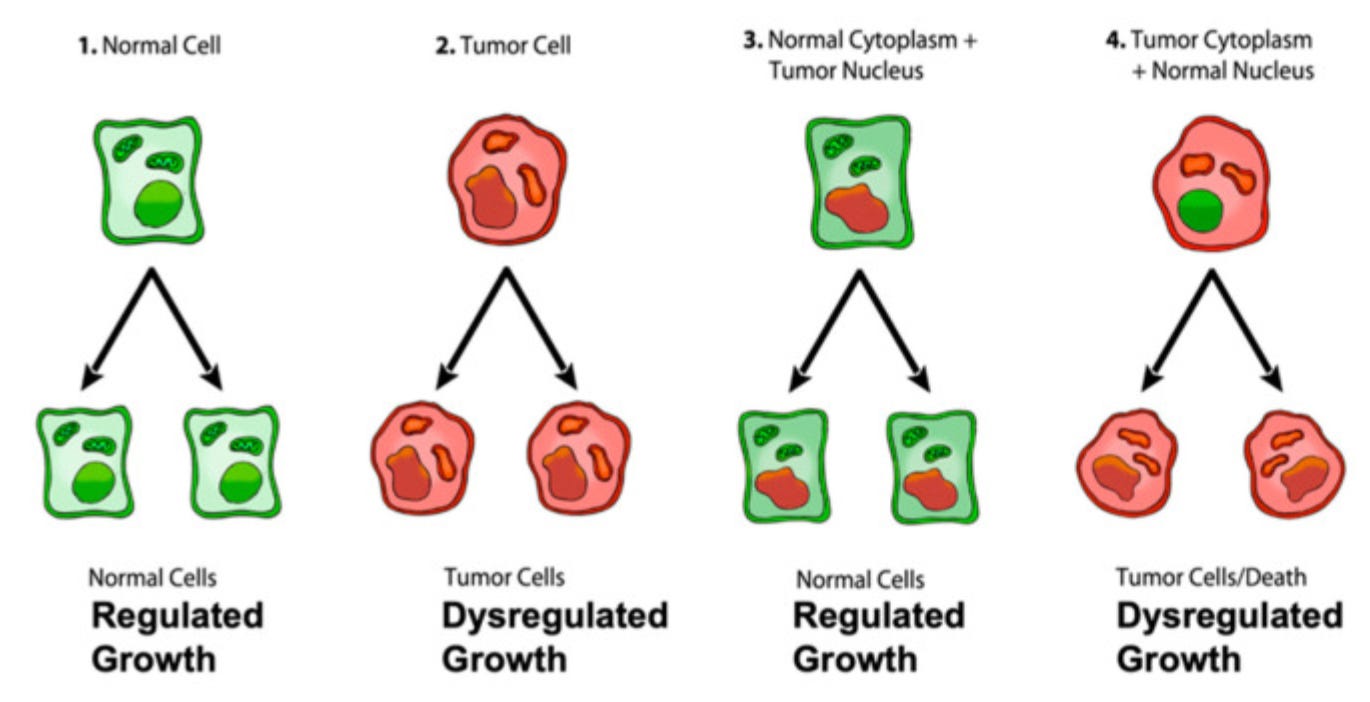
Cancer cells are in red; normal cells in green.
Obviously, cancer cells have dysregulated growth, while normal cells have regulated growth. The definition of cancer is basically growth gone wild. So in the graphic above, the green cell on the far left is normal and regulated and the red cell next to it is cancerous and has dysregulated reproduction.
When scientists remove the green nucleus from a normal cell and replace it with the red nucleus of a cancer cell—the nucleus contains the genetic material—the cell maintains its regulated division and growth as shown in the graphic second from the right. And note that these cells contain the cancer-associated genetic material in their nuclei.
But when green normal cell nuclei are transferred into red cancer cells, the cells either die or exhibit dysregulated growth.
The implication of all this is that it is not the genetic material in the nucleus that makes a cancer cell a cancer cell. It is instead the something in the cancer cytoplasm that does the trick. (Cytoplasm is the cell water and its contents other than the nucleus, so everything inside the cell except the nucleus — ie the mitochondria and all the other organelles inside the cell.)
The process shown in the graphic above has been replicated by numerous scientists.
In order to understand how the mitochondrial metabolic basis of cancer works, it’s necessary to get into the weeds of how we generate the energy that keeps us going. And it isn’t a simple process, so bear with me.
Life is a complex series of chemical reactions going on all the time. Most of them are driven by specific enzymes, which act as catalysts for chemical reactions that would normally not occur if left to their own devices. Were it not for enzymes, we would be giant lumps of chemicals just sitting around staring at one another. Enzymes make chemical reactions take place and speed them up.
Even with enzymes to catalyze these reactions, it requires energy to do so. Virtually all the energy the body uses to drive the reactions is coupled energy. Adenosine-triphosphate (ATP) is the body’s main coupler. When the phosphate bond in ATP is broken, the energy released is captured and used to drive the reaction in question. So if chemical A and chemical B which would normally never react with one another are brought together by a specific enzyme, ATP splits off a phosphate (P) to become Adenosine diphosphate (ADP) and provides the energy to drive the reaction.
So, when we eat, the energy derived from breaking the bonds in the fats, carbs, and protein ends up converting ADP back into ATP to be used as the body’s energy currency. We are constantly releasing energy to drive the countless reactions it takes to keep us alive by breaking down ATP to ADP. And we keep replenishing the ATP by using energy from food or stored fat or carbs or protein to convert the spent ADP back into ATP.
How much ATP do you think we make in a day?
It’s an amount about equivalent to our body weight! So, you can see we’re constantly using it and recharging it.
The how we do this is complex, but lies at the heart of the mitochondrial metabolic theory of cancer.
Everyone has heard of mitochondria, the little sausage-shaped organelles inside our cells that produce energy, the body’s energy factories. There are typically thousands of mitochondria in each cell, more in some than in others. And they’re all busy chugging away converting ADP into ATP.
But mitochondria aren’t the only places ATP is made. Some is made inside the cells but outside the mitochondria. One of the main ways in which ATP is generated outside of the mitochondria is via a process called glycolysis. It’s pretty inefficient compared to generating ATP in the mitochondria, but it has one advantage. Oxygen isn’t required for glycolysis, whereas it is for ATP to be generated in the mitochondria.
Since you can run out of oxygen during a heavy workout, you can continue thanks to glycolysis. It’s called going anaerobic, or without oxygen.
The process whereby ATP is generated in the mitochondria is complex. It’s not like glycolysis where enzymes and ADP come together to create an ATP.
For years very smart people knew that glycolysis and a few other reactions that threw off ATP were unable to meet the body’s needs. They all theorized that there was some cycle somewhere that would produce enough ATP to fuel the remainder. But despite very smart people searching for a long, long time, it took one of my intellectual heroes to figure it out. And when Peter Mitchell, who was a real iconoclast, did figure it out, no one believed him. It took a lot of work on his part to persuade other scientists that he was correct. He was ultimately vindicated and received the Nobel prize for his work.
(As an aside, I have a friend who worked in the lab right down the hall from the famous Nobel laureate Hans Krebs, who ferreted out the process that became known as the Krebs Cycle. My friend told me that Krebs told him the worst professional mistake he (Krebs) had ever made was not taking Peter Mitchell seriously. Krebs famously walked out of one of Mitchell’s lectures.)
Mitchell hypothesized that there was no other cycle that generated ATP. Instead he believed there was a membrane in the mitochondria—the inner mitochondrial membrane, to be exact—that ended up acting more or less like a battery. When bonds are broken in fats, carbs, and protein the energy is released as electrons, which get grabbed by electron carriers, and the energy contained in these electrons is used to drive protons—positively charged particles—to one side of the inner mitochondrial membrane (IMM).
As more and more protons are carried across the IMM, it ends up looking like this graphic from one of my presentation slides:
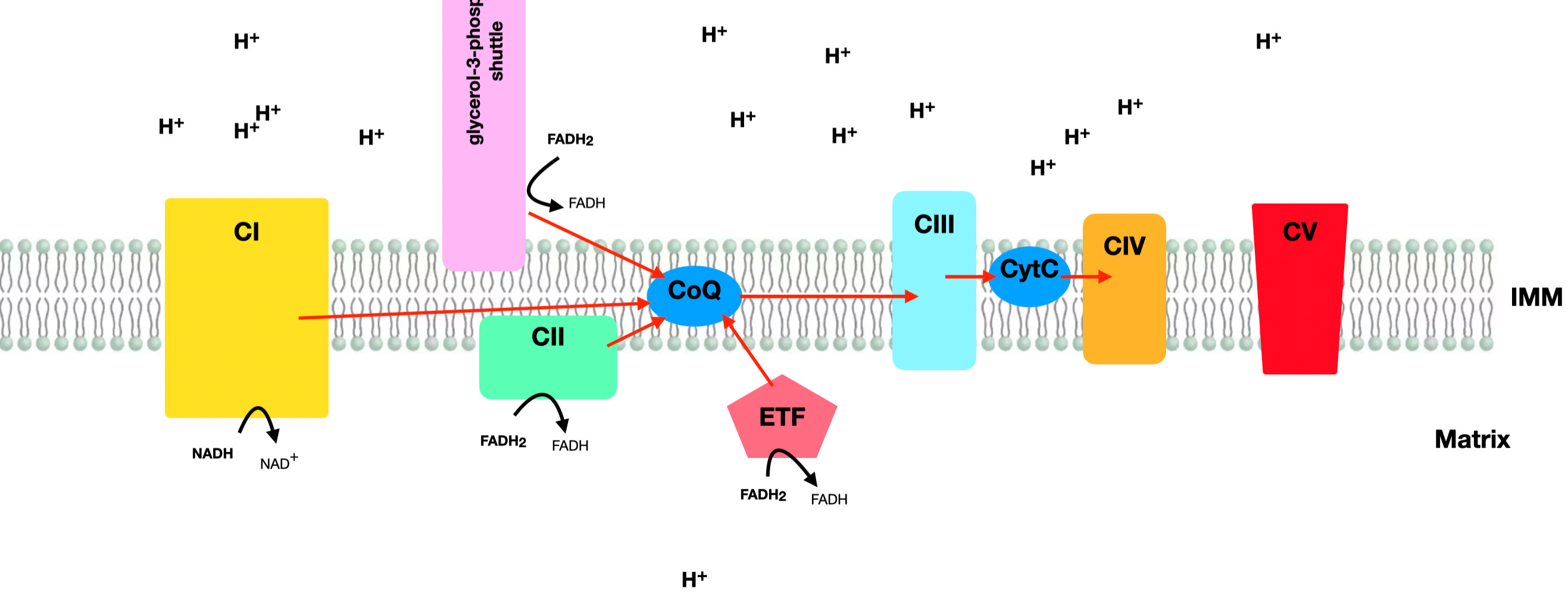
You can see all the positive charges (all those little H+s) above the IMM that have all been driven there by the high-energy electrons generated from fat, carbs, and protein. There is an imbalance of both electricity (positive charges) and hydrogen protons on the upper side of the IMM that exert both an electrical and chemical pressure across the membrane, much like water behind a dam. The hydrogens and the plus charges want to equalize across the membrane.
You can see the red sort of block at the right end of the IMM called CV, which stands for Complex 5. That is the opening which all these H pluses can rush through to get to the other side. Again, much like water behind a dam flowing through a turbine to generate electricity, these protons fly through Complex 5 and turn a tiny sort of turbine which converts ADP to ATP. This is how the vast majority of ATP is made. Probably in excess of 85 percent of our daily ATP is generated through this process that Peter Mitchell sussed out in what was basically a thought experiment to start.
At the end of this chain of electrons being transported in kind of bucket brigade fashion—called the electron transport chain—oxygen accepts them and converts to water. So, oxygen is required for this entire process to take place. No oxygen, no ability to run the electron transport chain.
The entire process operates to attach another phosphate (P) to ADP to convert it to ATP. The addition of a phosphate is called phosphorylation.
The entire process is called oxidative phosphorylation. Or OxPhos for short. Just to show you how powerful it is, one glucose molecule going through glycolysis throws off 2 ATP. The same glucose molecule going through OxPhos throws off somewhere between 30 and 36 ATPs.
So OxPhos yields vastly more energy (ATPs) than does glycolysis, which is a process called substrate-level phosphorylation or SLP. You’ll see these terms all the time in the literature, so now you understand what they mean.
Okay, that’s probably enough for one day. Or one week. Now that you understand how OxPhos works and how much more powerful it is than SLP in terms of generating energy, we can turn out attention next week to how cancer cells get their energy, the Warburg effect, and why a ketogenic diet works to help treat cancer.
Now let’s turn our attention to the latest conspiracy going around. If you’ve been reading this newsletter for a while, you should have picked up that I’m not much of a conspiracy theorist. I’m more a believer in Hanlon’s razor, which states "Never attribute to malice [or conspiracy] that which is adequately explained by stupidity." But sometimes I wonder.
Does the Ketogenic Diet Cause Heart Disease, Cancer, and Multiple Sclerosis?
This past week I received a couple of articles through Medscape, which is a subscription news site for doctors. (The general public can sign up as well. It’s free.) As you might imagine, Medscape hews pretty closely to the mainstream of medical thought. Over the past few years, I’ve read some positive articles on low-carb and ketogenic diets. So, I figured the tide might be turning, but this last couple of weeks has given me second thoughts.
I think the climate change folks are behind all this as they really want to get us all to quit eating meat.
Before I get into the meat of the discussion (pun intended), I’d like to show you a tiny bit of a 3 hr+ long podcast sent to me by a reader with Chris Palmer, a Harvard professor of psychiatry and a major proponent of the ketogenic diet for those with mental disorders, both severe and not so severe.
He was on the Andrew Huberman podcast. After Dr. Palmer had described all the positive results he had seen in various patients with a host of mental disorders talked turned to the use of the ketogenic diet for cognitive enhancement. Palmer recounted his experiences with subjects who had markedly improved cognition, and Huberman asked why more studies hadn’t been done. I’ve wondered the same thing myself. Palmer’s reply was quite enlightening. I’ve tee’d up the video below to the precise spot where he answers. It lasts maybe a minute.
So, now you know why more intensive studies haven’t been done in subjects with cognitive impairment.
You might think people with something more severe than cancer would stick in a study longer, but such is not the case. Here is a post I wrote several years ago about cancer patients who had gone through every treatment available, had been told nothing more could be done for them, and were offered the chance at a ketogenic diet. Most of them dropped out because they missed carbs. (Here is the most recent update I could find on the study.)
Getting back to the two studies I was fed on Medscape that involved the ketogenic diet and heart disease and the low-carb, high-fat diet and cancer and MS. What is amazing about these studies (if you want to call them that) is that there are thousands of medical studies published each month about all kinds of diseases, treatments, medications, supplements, etc. You name it, and it can be found in the medical literature. So with this cornucopia of material available why did Medscape focus on such a crappy poster on the ketogenic diet and heart disease? And the even crappier article about cancer and MS.
Let’s look deeper.
Not only did the editors of Medscape jump on this poster, but I found articles from CNN and the American College of Cardiology as well. The internet probably has a hundred more.
The first one about the ketogenic diet and heart disease was not a published study—it was a poster. Here’s how that works. Scientists, usually early in their training, do studies that they may have difficulty getting published. They end up putting their data on a poster and presenting it at a scientific meeting. Other scientists go to the poster presentations and ask questions and make comments. The budding scientists then learn how to deal with scientific criticism and what it’s like to be queried on their work. Usually the outfit putting on the conference will publish the posters in their journal, but they are not peer reviewed.
This poster was about a study done looking at subjects who had been on a low-carb, high-fat diet. Here’s how it starts off.
Consumption of a low-carbohydrate, high-fat diet, dubbed a "keto-like" diet, was associated with an increase in LDL levels and a twofold increase in the risk for future cardiovascular events, in a new observational study.
The fact that it is identified as an observational study tells you it isn’t worth much.
But the idea that the low-carb diet was associated with an increase in LDL is a real give away. The authors of this poster are assuming that LDL is a risk factor for heart disease, which it probably isn’t. The LDL relationship to heart disease is another one of those subjects that literally tens of millions (if not hundreds of millions) of dollars have been thrown at trying to prove a causal relationship to little effect. Going back to Pief Panofsky,’s law that "if you throw money at an effect and it doesn't get bigger, that means it's not really there." God only knows how much money has been thrown at trying to connect LDL with heart disease causally with nothing to show for it. Should tell you something. I can pretty accurately guess what Panofsky would have said about it.
There is another factor at play here as well. I wrote a blog post about this years ago.
What many people don’t realize is that LDL cholesterol almost always isn’t a measured parameter in a blood test. LDL is calculated, not measured directly. What is measured is total cholesterol, HDL-cholesterol, and triglycerides. Based on these measurements, LDL is calculated using the following formula developed by William Friedewalde over 50 years ago:
LDL = Total cholesterol - HDL - triglycerides/5
When Friedewald et al worked this out, they realized that if triglycerides were over 400 mg/dl the formula wouldn’t work. Which is why if you get a lab test back with triglycerides over 400, there will be a note saying that LDL could not be calculated.
What Friedewald et al didn’t look at is what happens if triglycerides are low—as they typically are in those following low-carb diets. Several studies have been published on this showing that when triglycerides are low, LDL can be overestimated by 20-40 mg/dl.
So, if the subjects in this poster presentation had elevated LDL levels, how high were they compared to those on the standard diet?
Levels of LDL were 3.80 mmol/L (147 mg/dL) in the keto-like group vs 3.64 mmol/L (141 mg/dL) in the standard group (P = .004).
I wouldn’t say that was an earth-shattering difference.
Also, I love how they call the diet a “keto-like” diet.
For the study, Iatan and colleagues defined a low-carbohydrate, high-fat diet as consisting of no more than 25% of total daily energy from carbohydrates and more than 45% of total daily calories from fat. This is somewhat higher in carbohydrates and lower in fat than a strict ketogenic diet but could be thought of as a 'keto-like' diet.
Why did they do this when 25 percent carbs is hardly a ketogenic diet? Probably because the ketogenic diet is so popular currently due to its effectiveness in treating a host of disorders. And for easy and fairly rapid weight loss.
How did the researchers determine that those on the “keto-like” diet developed heart disease at twice the rates of those on the standard diet?
You’ll love this. Here is what they came up with.
After an average of 11.8 years of follow-up, 9.8% of participants on the low-carbohydrate/high-fat diet vs 4.3% in the standard diet group experienced one of the events included in the composite event endpoint: angina, myocardial infarction, coronary artery disease, ischemic stroke, peripheral arterial disease, or coronary/carotid revascularization.
After adjustment for other risk factors for heart disease — diabetes, hypertension, obesity, and smoking — individuals on a low-carbohydrate, high-fat diet were found to have a twofold risk of having a cardiovascular event (HR, 2.18; P < .001).
Sounds pretty bad. How did they evaluate these subjects?
On enrollment in the Biobank, participants completed a one-time, self-reported 24-hour diet questionnaire and, at the same time, had blood drawn to check their levels of cholesterol. The researchers identified 305 participants whose questionnaire responses indicated that they followed a low-carbohydrate, high-fat diet. These participants were matched by age and sex with 1220 individuals who reported eating a standard diet. [My bold emphasis]
Here’s more info on the study population.
Of the study population, 73% were women and the average age was 54 years. Those on a low carbohydrate/high fat diet had a higher average body mass index (27.7 vs 26.7) and a higher incidence of diabetes (4.9% vs 1.7%). [My bold for emphasis]
So, these subjects were evaluated by a “one-time, self-reported 24-hour diet questionnaire,” and of the subjects in the keto-like diet group there was a more than double incidence of diabetes as compared to the control group.
Since diabetes is a major risk factor for heart disease, do you think that might have had something to do with the outcome?
You’ve got a population who provided a one-time dietary assessment, which tells you what diet they were following on that particular day. Of the ones who answered that they were on a keto-like diet, more than twice as many had diabetes as those not on a keto-like diet. And you're surprised that 11.8 years later, the group that had their diets identified on one particular day and who were diabetic developed more heart disease.
I hope the folks who did this Mickey Mouse study are sitting around awaiting a call from the Nobel Prize committee.
This is one of the sorriest pieces of dung I’ve ever seen. But there are a LOT of similar pieces of dung spread throughout the scientific literature. My question is why with all the decent studies to pick from Medscape would focus on this one?
It adds nothing to the sum of knowledge about anything.
The next study was even worse.
It’s not really even a study. It’s mere speculation based upon some idiotic reasoning.
The title is “Can Particles in Dairy and Beef Cause Cancer and MS?”
It uses the most specious reasoning to try to connect particles in beef with the development of cancer and/or MS forty years later. Here’s how it starts.
In our Western diet, dairy and beef are ubiquitous: Milk goes with coffee, melted cheese with pizza, and chili with rice. But what if dairy products and beef contained a new kind of pathogen that could infect you as a child and trigger cancer or multiple sclerosis (MS) 40-70 years later?
That’s right. What if?
And here is the data:
According to de Villiers and zur Hausen, there are good reasons to believe that other pathogens could cause chronic inflammation and thereby lead to cancer. Epidemiologic data suggest that dairy and meat products from European cows (Bos taurus) are a potential source. This is because colon cancer and breast cancer commonly occur in places where these foods are heavily consumed (ie, in North America, Argentina, Europe, and Australia). In contrast, the rate is low in India, where cows are revered as holy animals. Also noteworthy is that women with a lactose intolerance rarely develop breast cancer.
Oh, and this POS article was translated from the German version of Medscape. I guess we don’t have enough stupid studies in English to fill the pages, so Medscape has to troll the German literature.
Again, why publish this when there is so much decent literature out there.
I suspect both of these awful articles were somehow picked by climate change folks whose actual or self-imposed job it is to make us fear meat.
Okay, time for something pleasurable.
Video of the Week
This one is a for sure winner. I love this one more than I can say. Just sit back, listen, and enjoy! I’ve probably watched it twenty times so far.
Was I right? Did you enjoy it?
That’s about it for this week. I’ll be back next Thursday. Till then, keep in good cheer.
Before you go, take a look at what our sponsors have to offer. Dry Farm Wines, HLTH Code, and Precision Health Reports.
Dr. Eades, you're right about Dr. Fung's Cancer Code. But it gets criticized because people expect it to solve cancer for them and they get mad he is talking about route cause and history. Many people are of the "just tell me what to do!" mindset and don't care to understand how they got to where they are. That's the real issue. Yesterday, I was looking at my son's path slides as he studies for the STEP1 exam next month, and he showed me the slides for follicular thyroid cancer, which I had 7 years ago. I have been trying to understand why i developed thyroid cancer and never got an answer, but those slides made sense to me and suddenly I had an epiphany about cause. I went back into pubmed, and sure enough, I found a study that linked insufficient iodine intake with follicular thyroid cancer. And that made sense to me, a person who avoided salt my entire life because the Anti Salt Experts told us salt would kill us. Of course I didn't supplement with iodine either. I am pretty much done with The Experts. My endocrinologist, whom I love and respect, says nobody is iodine deficient in this country, but I don't know about that. The real issue with doctors is that they are so expert at niche areas they fail to understand that their body part is connected to the rest of the body and maybe their fix for one thing is destroying something else. Your discussion of ldl is spot on.
I love The Arrow. Confirmation bias? Maybe. I am just glad that I am not the only one thinking this way. Spend enough time watching msm and you wonder if you are the one standing on your head telling everyone they are upside down, or vice versa.
Excellent! Thanks for continuing the dive into cancer! Love the Video of the Week!