



The Arrow #140

Hello everyone.
Greetings from St. Andrews, Scotland.
Four days into our trip so far. A few observations.
We had a kind of circuitous route to get us to Edinburgh, where we started. We flew from Dallas to Boston, had a long layover during which we had to collect our bags and schlep them to another terminal. We then flew Aer Lingus to Dublin. It was only a five and a half hour flight, so after getting settled in and having dinner, there wasn’t a lot of time to sleep. Plus there was a fair amount of turbulence, which seemed to kick in just as I was starting to fall to sleep. I’m a pretty light sleeper, so whenever I would be just drifting off, the plane would jerk all over the place. Then I would have to start over.
We got to Dublin, then had to walk forever to get to our flight to Edinburgh. Short flight, but long wait for baggage. Then got driven to our hotel, The Scotsman, arriving at about 9:30 am. Of course, our room wouldn’t be ready until 3 PM, which meant we had to walk around Edinburgh for almost five hours.
We’ve been to Edinburgh a number of times over the years, but the one thing we haven’t done is visit the museum at the Royal College of Surgeons. We decided to give it a go. More about which in a bit.
We ended up back at the hotel at around 3 PM, got checked into our room, then fought off the urge to go immediately to bed. In our view, the best thing to do when heading for Europe is to stay awake until it is time to go to bed on European time. It’s a tough fight after being awake for 30 plus hours, but if you can do it and hit the hay at 10:30 PM or so, then you get on European time pretty quickly.
We did that. I slept like a rock for about seven hours. And woke up feeling great. Really great, in fact. Which got me thinking. And that’s all I’m doing here. The text equivalent to thinking out loud, which is always a dangerous thing to do on a public forum. But…
Sleep Fasting
You can’t stay awake forever. At some point, you’ve got to sleep. If not, you die. The same can be said about eating. You can go a long time without eating, but not forever. If you decide not to eat, you’ll ultimately die of starvation.
But going without food for a limited time is good for you. Study after study—both in animals and humans—has shown that intermittent fasting brings about many good effects. All kinds of good things happen including a bump in brain-derived neurotropic factor (BDNF), which increases brain plasticity along with a host of other beneficial effects.
After my sleep fast a couple of days ago, when I finally did sleep, I slept much more soundly than usual. And woke up feeling terrific. Much better than I usually feel after awakening from a typical night’s sleep. I felt well rested and hugely energetic.
It recalled many, many times during which I was on call and ended up spending the night awake in the operating room or dealing with one catastrophe after another all night long in the emergency room. When I thought back about those days, I recalled how dog tired I was when I was finally able to get to sleep after being awake 24-48 hours. And how terrifically rested and energetic I felt after awakening.
I don’t know why I didn’t think about it before, as I had certainly been sleepless for a day or two (once for four straight days) many times, but maybe doing the sleep version of intermittent fasting might be a good thing. I’m sure Paleo man ended up going sleepless periodically due to being on a long hunt or whatever. So, maybe a little sleep deprivation here and there—as long as followed by an opportunity for a good sleep after—might be as good a thing as intermittent food fasting.
This idea is total speculation on my part. I haven’t had the time to dig into the medical literature to see if there is anything to it. Or if anyone else might have made the same observation. All I know is that after awakening from about seven hours of solid, deep sleep following having stayed awake for about 35 hours straight, I felt spectacularly good. And hugely energetic.
Of course, we’re talking an n=1 here. MD did sleep on the plane. She is a much sounder sleeper than I, so she picked up a few hours of sleep on the plane that I didn’t get. When she awakened after we finally got to sleep in a real bed, she didn’t have the same experience as I did.
So, are sleep fasts here and there maybe a good thing? It’s a reasonable question. If anyone has any experience or knowledge on the subject, let me know.
Royal College of Surgeons Museum
While we were waiting for our room to be ready, we walked the half mile or so to the RCS Museum, which is housed along with the Wohl Museum of Pathology. I love to haunt museums like these because in them you can see pathology you don’t ever seen in medical practice today.
The world was a different place medically a century and a half ago. There was not a lot of early diagnosis, and even if an early diagnosis were made, there weren’t a lot of successful treatments to be had. Consequently, people lived with whatever they had until it killed them. Or something else did.
The Wohl Museum of Pathology is one exhibition case after another of specimens of disease categorized by the kind of disease or part of the anatomy.

The above is just a tiny fraction of the collection. I’m not sure it would be of great interest to a non-medical person because unless you kind of know what to look for, it’s difficult to see the pathology. These are old samples—most from the 1800s—from a time when the staining techniques were not the best, so everything is kind of monochromatic. But if you know what to look for, it is really incredible.
MD and I looked at every specimen. And, as I wrote earlier, the advanced pathology is something you just don’t see today. Most cancers are caught much earlier nowadays. And the trauma is much better dealt with. For example, one of the exhibits is of the crushed left hand of an adult male. He obviously worked in some sort of factory and something smashed his hand. His thumb and index finger were missing, and the third was damaged but salvageable. Today, he would have undergone reconstructive surgery, which would have left him not with a totally functional hand, but with a semi-functional one. When this happened to him 150 years ago, the treatment was amputation of the entire hand at mid-forearm. Which was what the specimen was: his amputated hand and lower arm.
Tremendous strides have been made in this kind of trauma surgery since the date of his injury. Had the severed fingers and thumb been brought in, they might have been salvaged today. But not then.
There were so many cases of advanced cancer. Situations you just never see today. There are bones completely filled with cancer. Same with multiple organs. Absolutely bursting with cancer.
Then there were the various organs that had been infected with one kind of infectious agent or another. You would probably never see infections this extensive today because of the advent of antibiotics.
All I could think of when looking at all these specimens is the magnitude of the pain and suffering experienced by these poor people. I can’t imagine how painful it would be to have all the bone marrow in a large bone replaced by a growing cancer and pressing outward on the bone. It would have been incredibly painful. And, at that time, there would be nothing to have been done other than take some sort of narcotic for pain relief.
I’m sure these samples represent just the tip of the iceberg of the total amount of pain and suffering experienced by the population at that time. It was overwhelmingly depressing just to think about it.
The other thing I noticed about all these specimens was how small the people were in those times, doubtless as a consequence of malnutrition. People were tiny as compared to today when almost anyone can get enough protein to build a decent sized body. Not so much back then. Even people who were well to do—and might even be a little portly—were not very tall.
On display was the coat of Joseph Lister, the guy who basically developed antisepsis. He was the size of an average sixth grader today. I know because one of my grandchildren is a whip-thin sixth grader, and he would have fit perfectly into the jacket.
The combination of lack of good nutrition, living in squalor, and primitive medical care led to a population of people riddled with parasites and prone to any infection that came along.
Which brings me to another point.
I’ve been getting emails from a number of people who don’t believe infectious diseases exist. They apparently believe that bacteria and viruses—if they even exist—are simply fellow travelers with humans and cause problems only if humans don’t take care of themselves, eat right, and exercise. From their emails, if I’m reading them correctly, they believe that good health will thwart all these bugs of one type or another. Coming down with some kind of infection doesn’t mean you’ve been attacked by a bacteria or virus; it means you haven’t taken care of yourself and thus allowed yourself to become susceptible to disease.
This little placard over a case of puerperal fever should be enlightening to these folks. I grabbed a photo of it with my phone right before I was admonished for taking photos. (I hadn’t seen the sign.)
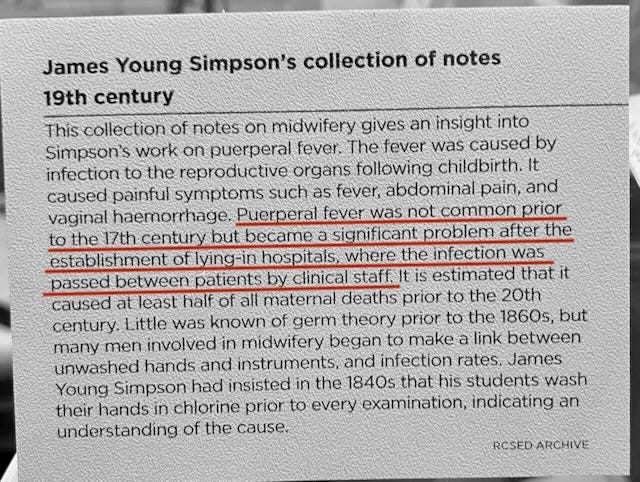
This was part of an exhibition showing the work of James Simpson (1811-1870), a Scottish doctor who figured greatly in the field of obstetrics.
Puerperal fever—a bad infection, often fatal, of the female genital tract after giving birth—was the bane of obstetricians back then. Women who gave birth with the help of midwives were not nearly as prone to these infections as were women who went to the hospital and were treated by obstetrical physicians.
Midwives typically worked with one mother at a time, whereas obstetricians had entire wards filled with postpartum women. This was before the germ theory of disease had been adopted, and the docs in the hospital would go from patient to patient spreading disease.
Before we get to how this happens, let me give you a fairly graphic explanation of what goes on in an obstetrical ward. I’m going to describe my own experience, which took place over 40 years ago, so I am clueless if this is how it is still done or not. But it was how it was done 40 years ago and back in the 1800s.
(Other than the time I spend on Ob-Gyn in med school, I haven’t really had any experience in obstetrics. I delivered one baby in an emergency room I was working in once. It came out fast, and I just more or less controlled the situation and delivered the placenta and all that goes with that. I am clueless as to how obstetrics is done today other than that most women get epidurals, which block most of the pain and unpleasantness.)
Since I doubt most readers of this newsletter have gone to medical school, let me explain a bit how it is structured. For the first two years of medical school, students are in the classroom learning all about anatomy, biochemistry, physiology and all the other basic medial sciences. When you’re through with these two years, you can name all the muscles and nerves and blood vessels and describe in detail all the biochemical pathways in the human body, including the enzymes that catalyze them. But you’re clueless as to how to diagnose, say, gall bladder disease.
That all happens in the third and forth years when you are on the wards taking care of patients hands on. It’s a big change in your life. You go from a nice classroom, and a short summer vacation, into being sometimes knee deep in gore. And you’re pretty much unprepared for it.
My first clinical rotation after the two years of classroom was obstetrics and gynecology. On my very first day, I was on call on labor and delivery.
I had done one pelvic exam in my life, and that was on a specially-trained nurse who hired herself out to medical schools to teach medical students how to do pelvic exams. She had had many such exams done on her and knew exactly how to talk a nascent doctor through doing one.
“Push harder. Don’t be afraid. If you don’t push harder, you’ll never be able to feel my ovaries.” It was that kind of instruction. And I was immensely grateful to have gotten it.
So, I head into my first day as a junior medical student (a JMS) on labor and delivery. In my medical school, there was nothing lower on the totem pole than a JMS. The JMSs did everything no one else wanted to do.
“Get a JMS over here to start an IV.” “Get a JMS over here to draw some blood.” It was one thing after another. The ward nurses lorded it over the JMSs. Everyone did. The JMSs were the whipping boys (and girls) of all the residents who were sleep deprived and overworked.
So, that’s what I walked into on my first day on labor and delivery.
I arrived in a ward with maybe six women in various stages of labor, some of whom are screaming at the tops of their lungs. “Give me something for the pain, please give me something for the pain.”
The resident in charge tells me I need to check these women for dilation and effacement periodically. The ones who haven’t been there all that long once an hour or so till they really get going. The ones who are closer to delivery, every 10-15 minutes.
At the time, I sort of know what dilation is, but I don’t have a clue as to what effacement is. I don’t dare ask and let anyone know I don’t know. So I find an obstetrics book in the little library on the ward and quickly read about it. And I realize I’m going to have to do a lot of pelvic exams on a lot of women, many of whom are thrashing and screaming, and they’re not going to tell me how to do it like the practice nurse who talked me through it.
I suspect very few readers of this section of today’s Arrow have had to stick their finger up a stranger’s vagina to measure cervical dilation and effacement, so an explanation is in order.
Take a look at the graphic below, which shows the progression of dilation and effacement. If you’re squeamish, you can skip on down.
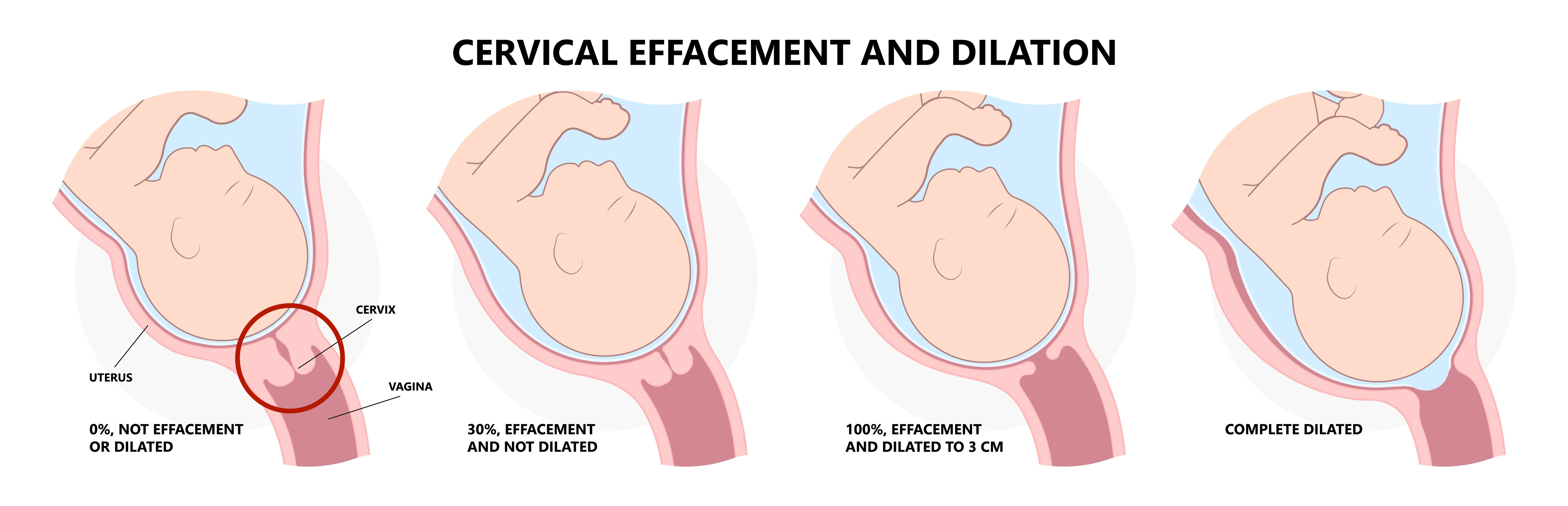
I’ve put a read circle around the graphic on the far left to show you the area of interest. The uterus is the muscular sack containing the baby who is working its way out. The vagina is the birth canal. (Which brings me to a real annoying nitpick I have. The vagina is not the external female genitalia. That is called the vulva. The vagina is the birth canal only. And now you now the difference.)
At the baby end of the birth canal within the red circle, you can see the cervix, which is the opening of the uterus through which the baby will ultimately come out. As you can see, it is an opening, but a thick one. Effacement is a guestimate by feel as to how thick this is from the vaginal end to the baby’s head end. You stick a couple of fingers of a gloved hand into the birth canal and stick one of the fingers in the opening of the cervix. You can tell by feel how thick the cervical tissue is. It gets thinner and thinner—i.e., more effaced—as delivery gets closer. It’s measured and put on the chart as a percentage of total effacement.
Once it’s effaced enough, you can feel inside the opening of the cervix and actually feel the baby’s head. Dilation is how open the hole is the baby is going to ultimately come through, and it’s measured and charted in number of centimeters.
Depending upon how many women are in labor, you can spend a lot of time just going from one to the next checking effacement and dilation. Each bed has a box of gloves on the table beside it. Often I would go to one bed, put on a glove, check the status, then peel off the glove, go to the next bed, put on a glove, and repeat. One after another. It doesn’t take too long before you’re pretty good at it.
Your reward for doing all this is to actually get to do a few deliveries. A skill you can be talked through.
One of my most vivid memories of that first day was lunchtime. It was so busy I couldn’t break for lunch, but the resident told me to go down, grab something from the cafeteria, and bring it up. I ran down and got my standard lunch, which was hog jowl and turnip greens with a side of fried okra. I was sitting there eating amidst the howls of a half dozen women, and all I could think of was how medieval the whole thing seemed.
Now take this same scene back to the early 1800s. Same situation. A ward full of women in labor, and a doctor going from one to another checking effacement and dilation. The only difference is that he isn’t using gloves. He’s just using his bare hands. And not washing them between patients. It’s almost inconceivable in today’s highly antiseptic world, but that was way back before anyone knew there were bacteria.
As you would expect, the doctors spread bacteria from anyone who harbored them to everyone else he did pelvics on.
But it even gets worse.
Back in those days, a lot of women got puerperal fever. Doctors diagnosed that much the same way they do female genital infections today: by doing a pelvic. But ungloved.Then they would go to their next patient and check her for effacement and dilation. And infect her.
And it was even worse than that.
Most of these doctors who worked on the wards did autopsies on their puerperal fever patients who died and would bring those bacteria to their patients in labor.
Is it any wonder that a large percentage of women died in these hospitals?
One Hungarian doctor named Ignaz Semmelweis (1818-1865) noticed that the maternity ward he ran in a Viennese hospital had vastly more deaths from puerperal fever than the ward run by midwives. He knew the midwives didn’t do autopsies on their patients who died—only the medical doctors did those.
Semmelweis reasoned that there might be something transferred from the corpses to the living women that caused the problem. He mandated that all doctors wash their hands with a chlorinated lime solution before examining a living women. The doctors went ballistic. They didn’t have time. (I’m sure they were as busy as I was on the maternity ward, but all I had to do was shuck off one pair of gloves and slip into another. If I had had to go through washing my hands with some sort of solution between exams, I suspect I would have felt ill used, too. Especially if I had been doing it without for years.)
But the proof of the pudding was in the fact that rates of puerperal fever dropped dramatically after the introduction of the washing after autopsies. Then Semmelweis made them start washing their hands between patients instead of just between autopsies and living patients. They complied and the rates of death fell even further.
However, that was a bridge too far. Despite the falling death rates, which one thinks would have gotten their attention, the doctors began screaming for Semmelweis’s head. He ultimately got canned, the hand washing ceased, and the rates of death from puerperal fever went back to their previous levels.
You would think the realization that the death statistics returning to pre-handwashing levels would have persuaded the doctors that Semmelweis might have been onto something. But, alas, such was not the case. It took many years before the germ theory took hold and puerperal fever pretty much vanished.
It’s somewhat similar to those today who continue to push the mRNA Covid vaccines despite the mountain of statistics showing they are neither safe nor effective. Some things never change.
Semmelweis was hounded to the point of a nervous breakdown. His colleagues had him institutionalized in an asylum, which was not a good place to be in the mid-1800s. While there he was beaten, and one of his cuts got infected. He died at age 47.
Remember this dreadful story next time someone tells you there is no such thing as a bacterium or a bacterial infection in a healthy person.
Let’s move on to something less awful.
Lallybroch and Castle Leoch
As I’ve mentioned before, I am on this trip to Scotland because my bride and the two friends she has infected with the TV series Outlander outvoted me. We had all planned to go to Italy, but now it is Scotland to see all the Outlander sights.
We saw a gracious plenty of them the third day we were here.
MD signed us up for an Outlander tour of areas around Edinburgh. Until I got sucked into going, I had no idea how popular this series is. We walked from our hotel to the bus station—maybe half a mile—to get on a tour mini-bus to spend an entire day going from one place to the next. There were God only knows how many tour buses queued up to take people on Outlander tours. There were a zillion people from all over the world—mainly Americans—lined up to go.
It was as dreadful as it sounds.
We kicked the tour off by going to Midhope Castle, which was portrayed as Lallybroch, the ancestral home of Jamie Fraser, the male lead of the show. The bus took us there and people were swarming in from all over. Once there, even though you’ve paid for the tour, it costs 6 pounds (~$7.50) to get in to see the place. For those of you who are fans, here is the photo I took.

I tried to grab a shot between tour buses so there wouldn’t be so many people. They were everywhere. All around the place and in the cave (fans will know what that means) and the dovecote people were swarming. It was unreal.
We ended up going all over the place and seeing a number of sites where the filming took place. I will bore you with only one more. Below is a photo of Doune Castle, which was portrayed as Castle Leoch in the series. All kinds of CGI work was done by the tech wizards to fill in missing pieces to make it look like it would have looked in the late 1700s. Here is how it looks now.

Sorry for the crappy photo. This is the side you see on the series, and it was into the sun.
This site was also swarming with people. As were they all.
Probably the worst part of the entire ordeal was the guy driving the bus and giving the patter about what we were seeing.
He talked like he had marbles in his mouth. You could just make out a word here and there.
It would be mumble, mumble, mumble, mumble, Mary Queen of Scots, mumble, mumble, mumble…and, ah..mumble, mumble, mumble…and etcetera (one of his favorite words) mumble, mumble, mumble…
You get the picture. The tour lasted from 9 am till 6 pm with a blessed hour for lunch. You can probably imagine my state of mind by the end of it. [The bride loved it though.]
French-Style Keto Cooking in Boulder, CO
One of my readers is the author (along with his wife) of a wonderful keto cookbook titled Bonjour Keto. It’s written in French and is a big hit in France. He sent me a copy of it, and it is excellent. I read enough French to understand it, and I can tell you it’s a heck of a book. He did all the photography, which is professional in quality, and his wife did all the cooking. The food looks spectacular. And the recipes are wonderful.
These fine folks now live in Boulder, Colorado, where MD and I had a practice for a few years. They have started a cooking school offering hands-on teaching to anyone who wants to learn French-style keto cooking. I have no affiliation with the school financial or otherwise. I’m just passing the info along at their request. If we were still living in Boulder, MD would be all over this, because I’m telling you, if you learn to cook keto like this, you will be the hero of the hive for sure.
Here is the link to their website describing the school.
Here is the Amazon link to their book in French from amazon.fr.
And here it is on amazon.com.
Fauci Returns
Fauci popped up on CNN a few days ago, thinking (I’m sure) that he was in friendly territory. The CNN talking head asked him about the mask issue and all the folderol getting started back up about the need to mask. The old Fauc was back in his element and immediately began to bullshit about how wonderful masks were and how much Covid they stop.
But then instead of swooning over the dulcet tones of the Fauc and thanking him ever so much for deigning to bring his bountiful expertise to CNN viewers, the talking head brought up the Cochrane report that said a review of all the studies on masks showed no evidence they prevented Covid.
The Fauc, needless to say, was caught off guard. How dare one of the minions from CNN question the great and powerful Fauci. And live on TV to boot. Fauci starts spouting this rambling word salad that means nothing. It’s truly hilarious.
For your viewing pleasure.
Fauci apparently doesn’t understand what a Cochrane report is. Scientists who are experts in both the subject under review and the ability to meticulously evaluate the scientific literature for validity review ALL the papers on a given subject and summarize the conclusions. In this case, scientists at Cochrane reviewed all the studies that had been done on masks and concluded there was no evidence masks—either cloth or N95—provide protection against Covid.
It’s fun to watch Fauci crawfish on live TV. Especially when what he says is meaningless.
Here is Maryanne Demasi’s take on it along with that of the lead author of the Cochrane report.

This video is so funny it will stand in as the Video of the Week as well.
As I mentioned last week, this issue and maybe the next one will be a little shorter than usual due to my travel situation. MD is the tour director on this outing, and she has been kind enough to include a little golf for me and the husband of the other couple we’re traveling with.
I got to play the Jubilee course at St. Andrews today. I shot an 87, but it was with rented clubs, not my own. And I had never played the course, which is considered to be the most difficult of all the St. Andrews courses.
One other thing…
New Covid Book
A couple of days ago a reader emailed me asking me if I had read the book Expired: Covid the Untold Story by Clare Craig. Not only had I not read it, I hadn’t even heard of it. I was able to download it on my Kindle and have gotten about a quarter of the way into it. It is terrific and fills all the gaps left by Turtles All The Way Down and Dissolving Illusions, two of my other favorite books. Very well written, easy to read, and filled with surprising information.
Okay, that’s about it this week. I’ll be back next Thursday from somewhere in Ireland. Until then, keep in good cheer.
Thanks for reading all the way to the end. If you got something out of it, please consider becoming a paid subscriber. I would really appreciate it.
Finally, don’t forget to take a look at what our kind sponsors have to offer. Dry Farm Wines, HLTH Code, Precision Health Reports,and The Hustle (free).
Dear Mike - I loved this edition of The Arrow, I’d have given it Fantabulous! if you had had a Poll ! I really enjoyed your "text equivalent to thinking out loud” - your thoughts on sleep, the Museum, and childbirth and the terrible infection rate in 1800's prior to doctors realising that infections passed from one patient to the other, your thoughts on the tour, all of it !
Doune Castle - I’ve never seen Outlander but as soon as I saw that photo you took of Doune Castle I thought Monty Python and the Holy Grail ! Sure enough I checked on the internet and lots of scenes in that film were done there including the absolutely hilarious scene, among many hilarious scenes, where King Arthur and Patsy are standing at the base of the wall asking the “French" knight who is on the castle battlements, who has the outrageously funny accent, to see the Holy Grail - one of the funniest scenes in the funniest of films.
Do Democrats have some mythical virus that has caused them to be 'like this.'
By that I mean to think that because Trump has been indicted ( formally accused - not convicted on anything...) he can't run for president? That they can enforce their view of 'science' on me even if it is false ( RE: Fauci, above). That even though carbon models of climate are not able to track the past they are grounds for setting policy today for the future... and reason to ban such things as incandescent light bulbs...maybe gas stoves...too. Does a mythical virus breed the idiocy that because we can see all the damage done by recent weather events we can order all this stupid stuff to be done in the name of stopping CLIMATE CHANGE- when best science says it is not the real reason?? And Still Biden promotes oil drilling for Iran and Venezuela...and DOES not NOT ban or highly tax US imports form Carbon spewing economies like China? and India Orrr.... If climate change is really an exigent threat (as about 1,000 PhDs just said it wasn't) but if it is and they are wrong...why aren't we taking more dramatic steps? All this needs to be explained it is illogical. ( not Spock-like). If carbon is the reason then we need a better electric grid yesterday....instead we are doing little today. We need green fuel to fire it up...the only ONLY choice on a large scale as MUST bee needed (if you believe...) is nuclear yet. No no no. we do not do that. OK so how does it make sense to let the planet boil and die instead of creating nuclear fuel and spent rods we cannot recycle now but that we might be able to in the future. to SAVE THE PLANET FOR EXCESS CARBON NOW?? Should we really let the planet burn festooned with solar panels (made in carbon-spewing China) and windmills? ( with all those windmills sticking out, from Outer Space the earth will look like the corona virus!!) Surely this 'thinking' is the result of some new unchecked disease. Healthy Democrats can't really think all this makes any sense....and then there is the recent paper here->> https://co2coalition.org/news/two-princeton-mit-scientists-say-epa-climate-regulations-based-on-a-hoax/ by two real scientists calling the carbon paradigm a hoax. They feature a plot of the 'carbon models and how poorly they fit data. clearly you must have BRAIN DAMAGE to use those models as a basis for policy... and now there is the return of Covid - just in time for the upcoming elections season and more mail in ballots form Venus and mars!!! . Joe Biden who cannot tell his left shoe from his right one- is already saying there is a new vaccine and this one will work!! (1) He can't know that and (2) AH HA..a tacit admission that the other ones did not work! and finally...Please do not ban guns. I may soon need to ask someone to shoot me and put me out of my misery... B